Richard Abraham's Myeloma Journey With the Elephant on His Back
By Richard Abraham
Since starting our love affair in 1996, my wife Stephanie and I have shared a passion for travel and adventure. In 2017, having been married for 18 years, we visited Shanghai, Thailand, Laos and Cambodia. The adventures in each venue could fill many pages, but those stories are for another day.
In 2017 I was a healthy 72-year-old. My only daily meds were one baby aspirin and a 10mg Lipitor. I had stopped smoking on April 11, 2003 and all bloodwork was normal. We exercised regularly. While in Cambodia along the Mekong River, in 95 degree heat, we had climbed 305 steps to visit a cave with hundreds of discarded broken Buddhas. Again, a story for another day.
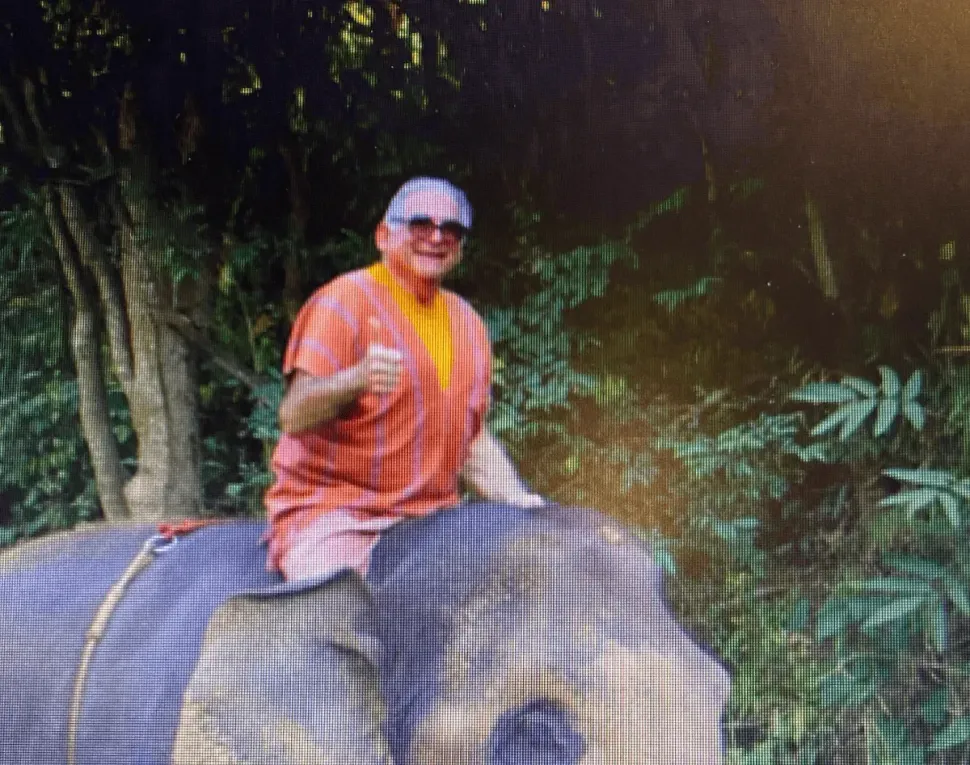
While in Thailand, we spent a half-day at an elephant rescue facility near Chang Mai. We were each assigned an elephant and a trainer. In addition to learning the elephant’s name, we learned commands to have them walk, stoop and kneel down so we could climb aboard, and fascinating facts about elephants (did you know that they only sweat between their toes?). After we each scrubbed our elephant with a large brush, we climbed on for a 45 minute bareback ride, holding only a rope. Stephanie’s elephant was 16 months pregnant – but again, that story is for another day.
When descending from my elephant, I thought I strained a hip abductor muscle. Minor discomfort, but it affected my walking. Quick trip to a pharmacy in Chang Mai resulted in being given 20 tramadol (synthetic opioid) without having seen a doctor or getting a Rx. Again, a story for another day.
Now back in the USA, the hip pain subsided in a week or so, but I started with lower back pain, which was very unusual for me. My doctor of 25 years said my back pain was caused by gait disturbance due to the hip muscle strain. He prescribed PT and anti-inflammatory meds.
After a couple weeks with no improvement, I went back to him seeking an MRI to see what was wrong. He initially refused, insisting that the problem was soft tissue, and that he could not medically justify to Medicare the cost of an MRI. Fortunately, I had brought Stephanie along, and she knew something more must be wrong, and insisted that he order it. His reply was “What are you worried about, it’s not going to show cancer!!”
Because he knew I was a reliable patient, and more so because of Stephanie’s insistence, the MRI was ordered. It was performed on the next day, Tuesday April 4, 2017, and I took the disc with me from the imaging center. The next day, in my office (I’m a lawyer who has dealt with personal injury matters for over 45 years, including many spinal injuries) I put the disc in my computer and looked at the MRI images. I saw something very peculiar in my lumbar spine. It looked like a vertebra (not the disc) was bulging out into the spinal canal and pressing on the spinal cord. I took the disc to my doctor’s office that day. The next morning, Thursday, I got a call from his office saying that they had made an appointment with an orthopedic surgeon for 3:00pm that day because I had a collapsed L1 vertebra, and other bony lesions in my spine and pelvis, making it look like I might have multiple myeloma. YIKES!!! What is that???
Our lives were instantly turned upside down. Despite our mantra always having been “Shame on you if you don’t enjoy every day,” this was a hard day to enjoy. Spine surgery? Cancer? How long have I had it? How long do I have to live? Damn that elephant who caused this injury!!! Ultimately we came to thank the elephant, for without the minor injury that eventuated in my diagnosis, the myeloma could have festered for another year without treatment.
We had trouble even starting to comprehend the true seriousness of my condition. At the surgeon’s office on Thursday we got the news that, because of a risk of spinal cord injury, he wanted me to be immediately admitted for pre-surgery testing, that I would stay over the weekend and that surgery would be scheduled for 6:30AM on Monday, April 10. I needed a spinal fusion, but until more testing he did not know if it would be a 3-level (T12-L2) or a 5-level (T11-L3) fusion.
But wait, we had plans for a dinner party at our house for 10 people the next night!! Friends had won a chef’s dinner at a silent auction and, because they loved our home, they wanted the party there. Therre was no way to postpone that. The lawyer in me then negotiated the following with the surgeon:
1. I would stay in the hospital overnight to get imaging and pre-op lab work;
2. I was guaranteed to be able to leave by 4:30 on Friday for the dinner party, but agreed to wear a hard plastic “clam-shell” device at all times except when sleeping;
3. I was not allowed to cook or do ANYTHING except sit in a chair or be in bed all weekend;
4. After the dinner party I would not drink any more wine before surgery.
Stephanie and I were in the initial stage of GRIEF, which is denial. If we had been able to appreciate the true seriousness of the collapsed vertebra, I would have stayed in the hospital. We had been in shock, and it was only months later that we became able to enjoy and even laugh about these events.
Surgery took 7 hours. They went in from the front and the back, and I have 2 lovely scars, each about 8” long. I have an internal titanium “cage” stabilizing my spine. I showed my younger son an x-ray, and he said “Dad, did you know you swallowed something really big – and it’s still there!”
Fortunately, I remember nothing of the first 3 days after surgery. Sadly, Stephanie has indelible nightmarish memories. One of them involves me being mechanically hoisted (like a horse out of quicksand) to go to radiology for a CT scan. Nevertheless, she stepped up to the plate as a spectacular caregiver and savior. One example: on Wednesday afternoon, the second day after surgery, two young women came into my hospital room and introduced themselves as physical therapists. They said they were there to start my physical therapy. I replied, “I don’t really feel like it today”, and they smiled and walked out saying they would see me “tomorrow”. Stephanie followed them out into the hall and said “Are you kidding me? You are letting that drugged up patient tell you ‘no’? If he is supposed to start PT today, put on your big girl panties and go back in there and explain to him what you want to do.” So they did, and I gladly walked with them once around the hospital floor.
The lesson here is that, in addition to a myeloma specialist, it is critically important to have a loving, attentive, educated and assertive caregiver. Having something explained simply as “walking once around the hospital floor” instead of “physical therapy” made all the difference that was required for me to willingly comply.
Support of family is also critical to a successful myeloma journey. My sons came to Philadelphia from Brooklyn and Chicago while I was still hospitalized after spinal surgery. Just their presence, in addition to their help and caring, eased my journey. My surgeon, Vincent Arlet, MD, had done such a great job that by December 2018, only 20 months after the surgery, Stephanie and I were able to travel to Panama for a wonderful two-week vacation with the Chicago family. No back pain and no limitation of movement. A true blessing! Being able to swim in the ocean, hike with the family and sail through the Panama Canal surely helped forget that I had cancer. Then, in the summer of 2019, the entire group of two sons, two daughters-in-law, and six grandchildren spent ten days with us in Switzerland and Lake Como, Italy. Returning to travel with family was surely the best medicine.
The bone marrow biopsy done during surgery, as well as blood work, confirmed the diagnosis of multiple myeloma. My Kappa Free Light Chains (KFLC) were over 8000 (normal is less than 19, and that’s not “thousands”). I was referred to Ed Stadtmauer, MD, a world-renowned myeloma specialist at UPENN, and immediately started on triplet drug therapy (Revlimid, Velcade and Dexamethasone) as well as Zometa for bone hardening.
Having never even heard of multiple myeloma, and being crushed by the word CANCER, it was doubly devastating to find out it’s a “bone marrow” cancer. That’s not something you can just cut out and cure. However, my research soon revealed the beginning of the good fortune and great karma that would accompany me on this journey. Genetic analysis of my bone marrow revealed that I had a t(11:14) genetic “translocation” which is associated with better outcomes than many other iterations of myeloma. I was so fortunate to be diagnosed in 2017 after so many advances in treatment with new medications being approved every year. I was also very fortunate that my body reacted well to the prescribed medications with minimal side effects. My KFLC number plummeted down by 95% (from 8000 to 400) in just four months.
The process of coming to terms, physically and emotionally, with being diagnosed with cancer and learning that there is no cure, is a life altering event. How will this affect the relationship with my wife? How do I tell my children? How will I react to their involvement, or lack of involvement, in my physical and emotional struggles? How much should I burden them with any details of this disease? How will this change how I view myself? How others view me? How will this change my working as a lawyer? Will other lawyers view me as “weakened”? The flood of questions and conflicting emotions was overwhelming – and I was just in the first month of a life-long struggle. I cannot overstate the extreme significance of establishing a relationship with a therapist or psychologist. The ability to have a professional interested in only one thing – my emotional welfare – made the journey so much more tolerable. To have a “safe space”, where overwhelming fears and emotions, frustrations, challenges and family dynamics can all be explored was so comforting. At first I saw my psychologist weekly, and I now continue to see her monthly.
Although “standard of care treatment” involves autologous stem-cell transplant after initial good response to medications, extensive discussion with my myeloma specialist led to Stephanie and me deciding to just collect and store the stem cells and defer the transplant. Many considerations informed that decision:
1. Although 72-years-old, I was still working full-time and did not want to interrupt work for 3 months;
2. With the t(11:14) translocation, combined with my excellent response to the initial medications, my prognosis was good;
3. I could elect to have transplant in 2-3 years, if needed. The other side of that coin, however, was that I would need to be healthy enough at that time to be eligible for transplant;
4. Although length of “progression free survival” was shorter without transplant, research indicated no difference in overall life expectancy.
After 2 years of stable bloodwork, my KFLC began to creep upward, indicating relapse into active myeloma. My hematologist and I agreed on a second opinion consult at Sloan Kettering in NY which resulted in a new triplet drug protocol – Carfilzomib, Pomalidomide and Dex. Although that treatment regimen knocked me on my butt with fatigue and shortness of breath, it brought my KFLC numbers down to NORMAL in 2 months! Reduced dosage of medications greatly alleviated side effects without interfering with the beneficial effects of the drugs. After 5 months on that drug protocol, with KFLC “normal” for 3 months, I had a bone marrow biopsy which revealed the miracle of MRD NEGATIVE STATUS – meaning nada, none, no detectible disease, entitling me to stop all meds.
I must emphasize the importance of getting a second opinion consultation. Dr. Stadtmauer was 100% in favor of my getting a second opinion because he knows that each patient is unique, and that there is no recipe or standard formula for treating this pernicious disease.
As is customary with this incurable disease, after 20 months off all medications, my KFLC started creeping up again. After six months of steadily rising KFLC numbers, the decision was made that I needed a new drug regimen. I was again so fortunate that the preferred drug, daratumumab (Darzalex) had recently been approved as a monthly injection, instead of as an infusion. Dara is often prescribed along with pomalidomide. I was scheduled to start these drugs in December 2020.
Due to our “wonderful” prescription drug and insurance industries, that meant I would need to pay $4500 co-pay in December, and $4500 again in January, a new “prescription year” under my plan. My doctor decided to delay starting pomalidomide for a month and just monitor how I responded to the dara. Surprise, surprise, within 6 weeks my KFLC was back to normal. Therefore, decision was made to defer starting the pomalidomide until I needed it. Another example of my good fortune and great karma, the need to take pomalidomide now was circumvented. I have now been only on Dara for 16 months, with stable bloodwork indicating “remission”. If KFLC starts climbing, the plan is to start pomalidomide in hopes that it will return me to remission. If it doesn’t, there are many other available treatment options – with more being developed every month.
The lesson here is that customary and “standard of care” drug protocols, which are based on good science and studies, are not the ONLY way of treating this strange disease. We each must become educated about our genetic makeup and the individuality of our disease. Even then, the importance of care by a myeloma specialist, obtaining a second opinion for major treatment decisions, and the loving attention of a caregiver, are critical factors in maintaining the best possible level of care to achieve and then maintain remission.
Early in this journey, because of personal fear and ignorance about this disease, I reached out to the Philadelphia Multiple Myeloma Networking Group (PMMNG). At the first meeting I felt so welcomed and comfortable to be among fellow myeloma patients and their care givers who were all so willing to share their experiences and provide reassurance that we could safely embark on a lifelong journey to overcome this disease. Some group members have been living with myeloma for 18, 22 and even 27years! I now have many new friends and a community that I know and trust to be able to help me and Stephanie through whatever and wherever this disease will take us.
Coming to accept that I have an incurable disease was no small task. Living with myeloma requires PATIENCE and acquiring patience has made my journey much easier. At first, after each monthly blood draw, until I saw the results indicating that my disease was still stable, I used to have significant anxiety. Is this the month that my numbers will skyrocket? Will there be any treatment effective for me? I have come to learn that, although relapse and rising KFLC numbers are an inevitable reality, there is a constant stream of new drugs available for effective treatment. I have also learned from one of my sons – “Why worry until there is really something to worry about?”
I think it is also beneficial to have defined goals. My first goal after diagnosis was to live to attend my oldest grandchild’s Bar Mitzvah which was 2 years ago. Since then, 2 more grandchildren have celebrated their Bar Mitzvahs. The next celebration will be in June 2022, the Bat Mitzvah of my only granddaughter. After the celebrations of the Bar Mitzvahs of my last two grandsons in 2025 and 2029, I will need to search for a new goal. As I learned several years ago, “I may have myeloma, but myeloma doesn’t have me!!”
Having a wife/partner/caregiver intimately involved in my myeloma journey has not only made the journey easier, but has also brought us closer. Stephanie and I are fortunate to have been able to resume travelling – especially with family members. In August 2022 we will take son, daughter-in-law and their three children to the National Parks at the Grand Canyon, Bryce and Zion, as well as a Navajo guided tour of Monument Valley.
We have truly returned to the original mantra of our relationship – “Shame on you if you don’t enjoy every day!”
By Richard Abraham
Since starting our love affair in 1996, my wife Stephanie and I have shared a passion for travel and adventure. In 2017, having been married for 18 years, we visited Shanghai, Thailand, Laos and Cambodia. The adventures in each venue could fill many pages, but those stories are for another day.
In 2017 I was a healthy 72-year-old. My only daily meds were one baby aspirin and a 10mg Lipitor. I had stopped smoking on April 11, 2003 and all bloodwork was normal. We exercised regularly. While in Cambodia along the Mekong River, in 95 degree heat, we had climbed 305 steps to visit a cave with hundreds of discarded broken Buddhas. Again, a story for another day.
While in Thailand, we spent a half-day at an elephant rescue facility near Chang Mai. We were each assigned an elephant and a trainer. In addition to learning the elephant’s name, we learned commands to have them walk, stoop and kneel down so we could climb aboard, and fascinating facts about elephants (did you know that they only sweat between their toes?). After we each scrubbed our elephant with a large brush, we climbed on for a 45 minute bareback ride, holding only a rope. Stephanie’s elephant was 16 months pregnant – but again, that story is for another day.
When descending from my elephant, I thought I strained a hip abductor muscle. Minor discomfort, but it affected my walking. Quick trip to a pharmacy in Chang Mai resulted in being given 20 tramadol (synthetic opioid) without having seen a doctor or getting a Rx. Again, a story for another day.
Now back in the USA, the hip pain subsided in a week or so, but I started with lower back pain, which was very unusual for me. My doctor of 25 years said my back pain was caused by gait disturbance due to the hip muscle strain. He prescribed PT and anti-inflammatory meds.
After a couple weeks with no improvement, I went back to him seeking an MRI to see what was wrong. He initially refused, insisting that the problem was soft tissue, and that he could not medically justify to Medicare the cost of an MRI. Fortunately, I had brought Stephanie along, and she knew something more must be wrong, and insisted that he order it. His reply was “What are you worried about, it’s not going to show cancer!!”
Because he knew I was a reliable patient, and more so because of Stephanie’s insistence, the MRI was ordered. It was performed on the next day, Tuesday April 4, 2017, and I took the disc with me from the imaging center. The next day, in my office (I’m a lawyer who has dealt with personal injury matters for over 45 years, including many spinal injuries) I put the disc in my computer and looked at the MRI images. I saw something very peculiar in my lumbar spine. It looked like a vertebra (not the disc) was bulging out into the spinal canal and pressing on the spinal cord. I took the disc to my doctor’s office that day. The next morning, Thursday, I got a call from his office saying that they had made an appointment with an orthopedic surgeon for 3:00pm that day because I had a collapsed L1 vertebra, and other bony lesions in my spine and pelvis, making it look like I might have multiple myeloma. YIKES!!! What is that???
Our lives were instantly turned upside down. Despite our mantra always having been “Shame on you if you don’t enjoy every day,” this was a hard day to enjoy. Spine surgery? Cancer? How long have I had it? How long do I have to live? Damn that elephant who caused this injury!!! Ultimately we came to thank the elephant, for without the minor injury that eventuated in my diagnosis, the myeloma could have festered for another year without treatment.
We had trouble even starting to comprehend the true seriousness of my condition. At the surgeon’s office on Thursday we got the news that, because of a risk of spinal cord injury, he wanted me to be immediately admitted for pre-surgery testing, that I would stay over the weekend and that surgery would be scheduled for 6:30AM on Monday, April 10. I needed a spinal fusion, but until more testing he did not know if it would be a 3-level (T12-L2) or a 5-level (T11-L3) fusion.
But wait, we had plans for a dinner party at our house for 10 people the next night!! Friends had won a chef’s dinner at a silent auction and, because they loved our home, they wanted the party there. Therre was no way to postpone that. The lawyer in me then negotiated the following with the surgeon:
1. I would stay in the hospital overnight to get imaging and pre-op lab work;
2. I was guaranteed to be able to leave by 4:30 on Friday for the dinner party, but agreed to wear a hard plastic “clam-shell” device at all times except when sleeping;
3. I was not allowed to cook or do ANYTHING except sit in a chair or be in bed all weekend;
4. After the dinner party I would not drink any more wine before surgery.
Stephanie and I were in the initial stage of GRIEF, which is denial. If we had been able to appreciate the true seriousness of the collapsed vertebra, I would have stayed in the hospital. We had been in shock, and it was only months later that we became able to enjoy and even laugh about these events.
Surgery took 7 hours. They went in from the front and the back, and I have 2 lovely scars, each about 8” long. I have an internal titanium “cage” stabilizing my spine. I showed my younger son an x-ray, and he said “Dad, did you know you swallowed something really big – and it’s still there!”
Fortunately, I remember nothing of the first 3 days after surgery. Sadly, Stephanie has indelible nightmarish memories. One of them involves me being mechanically hoisted (like a horse out of quicksand) to go to radiology for a CT scan. Nevertheless, she stepped up to the plate as a spectacular caregiver and savior. One example: on Wednesday afternoon, the second day after surgery, two young women came into my hospital room and introduced themselves as physical therapists. They said they were there to start my physical therapy. I replied, “I don’t really feel like it today”, and they smiled and walked out saying they would see me “tomorrow”. Stephanie followed them out into the hall and said “Are you kidding me? You are letting that drugged up patient tell you ‘no’? If he is supposed to start PT today, put on your big girl panties and go back in there and explain to him what you want to do.” So they did, and I gladly walked with them once around the hospital floor.
The lesson here is that, in addition to a myeloma specialist, it is critically important to have a loving, attentive, educated and assertive caregiver. Having something explained simply as “walking once around the hospital floor” instead of “physical therapy” made all the difference that was required for me to willingly comply.
Support of family is also critical to a successful myeloma journey. My sons came to Philadelphia from Brooklyn and Chicago while I was still hospitalized after spinal surgery. Just their presence, in addition to their help and caring, eased my journey. My surgeon, Vincent Arlet, MD, had done such a great job that by December 2018, only 20 months after the surgery, Stephanie and I were able to travel to Panama for a wonderful two-week vacation with the Chicago family. No back pain and no limitation of movement. A true blessing! Being able to swim in the ocean, hike with the family and sail through the Panama Canal surely helped forget that I had cancer. Then, in the summer of 2019, the entire group of two sons, two daughters-in-law, and six grandchildren spent ten days with us in Switzerland and Lake Como, Italy. Returning to travel with family was surely the best medicine.
The bone marrow biopsy done during surgery, as well as blood work, confirmed the diagnosis of multiple myeloma. My Kappa Free Light Chains (KFLC) were over 8000 (normal is less than 19, and that’s not “thousands”). I was referred to Ed Stadtmauer, MD, a world-renowned myeloma specialist at UPENN, and immediately started on triplet drug therapy (Revlimid, Velcade and Dexamethasone) as well as Zometa for bone hardening.
Having never even heard of multiple myeloma, and being crushed by the word CANCER, it was doubly devastating to find out it’s a “bone marrow” cancer. That’s not something you can just cut out and cure. However, my research soon revealed the beginning of the good fortune and great karma that would accompany me on this journey. Genetic analysis of my bone marrow revealed that I had a t(11:14) genetic “translocation” which is associated with better outcomes than many other iterations of myeloma. I was so fortunate to be diagnosed in 2017 after so many advances in treatment with new medications being approved every year. I was also very fortunate that my body reacted well to the prescribed medications with minimal side effects. My KFLC number plummeted down by 95% (from 8000 to 400) in just four months.
The process of coming to terms, physically and emotionally, with being diagnosed with cancer and learning that there is no cure, is a life altering event. How will this affect the relationship with my wife? How do I tell my children? How will I react to their involvement, or lack of involvement, in my physical and emotional struggles? How much should I burden them with any details of this disease? How will this change how I view myself? How others view me? How will this change my working as a lawyer? Will other lawyers view me as “weakened”? The flood of questions and conflicting emotions was overwhelming – and I was just in the first month of a life-long struggle. I cannot overstate the extreme significance of establishing a relationship with a therapist or psychologist. The ability to have a professional interested in only one thing – my emotional welfare – made the journey so much more tolerable. To have a “safe space”, where overwhelming fears and emotions, frustrations, challenges and family dynamics can all be explored was so comforting. At first I saw my psychologist weekly, and I now continue to see her monthly.
Although “standard of care treatment” involves autologous stem-cell transplant after initial good response to medications, extensive discussion with my myeloma specialist led to Stephanie and me deciding to just collect and store the stem cells and defer the transplant. Many considerations informed that decision:
1. Although 72-years-old, I was still working full-time and did not want to interrupt work for 3 months;
2. With the t(11:14) translocation, combined with my excellent response to the initial medications, my prognosis was good;
3. I could elect to have transplant in 2-3 years, if needed. The other side of that coin, however, was that I would need to be healthy enough at that time to be eligible for transplant;
4. Although length of “progression free survival” was shorter without transplant, research indicated no difference in overall life expectancy.
After 2 years of stable bloodwork, my KFLC began to creep upward, indicating relapse into active myeloma. My hematologist and I agreed on a second opinion consult at Sloan Kettering in NY which resulted in a new triplet drug protocol – Carfilzomib, Pomalidomide and Dex. Although that treatment regimen knocked me on my butt with fatigue and shortness of breath, it brought my KFLC numbers down to NORMAL in 2 months! Reduced dosage of medications greatly alleviated side effects without interfering with the beneficial effects of the drugs. After 5 months on that drug protocol, with KFLC “normal” for 3 months, I had a bone marrow biopsy which revealed the miracle of MRD NEGATIVE STATUS – meaning nada, none, no detectible disease, entitling me to stop all meds.
I must emphasize the importance of getting a second opinion consultation. Dr. Stadtmauer was 100% in favor of my getting a second opinion because he knows that each patient is unique, and that there is no recipe or standard formula for treating this pernicious disease.
As is customary with this incurable disease, after 20 months off all medications, my KFLC started creeping up again. After six months of steadily rising KFLC numbers, the decision was made that I needed a new drug regimen. I was again so fortunate that the preferred drug, daratumumab (Darzalex) had recently been approved as a monthly injection, instead of as an infusion. Dara is often prescribed along with pomalidomide. I was scheduled to start these drugs in December 2020.
Due to our “wonderful” prescription drug and insurance industries, that meant I would need to pay $4500 co-pay in December, and $4500 again in January, a new “prescription year” under my plan. My doctor decided to delay starting pomalidomide for a month and just monitor how I responded to the dara. Surprise, surprise, within 6 weeks my KFLC was back to normal. Therefore, decision was made to defer starting the pomalidomide until I needed it. Another example of my good fortune and great karma, the need to take pomalidomide now was circumvented. I have now been only on Dara for 16 months, with stable bloodwork indicating “remission”. If KFLC starts climbing, the plan is to start pomalidomide in hopes that it will return me to remission. If it doesn’t, there are many other available treatment options – with more being developed every month.
The lesson here is that customary and “standard of care” drug protocols, which are based on good science and studies, are not the ONLY way of treating this strange disease. We each must become educated about our genetic makeup and the individuality of our disease. Even then, the importance of care by a myeloma specialist, obtaining a second opinion for major treatment decisions, and the loving attention of a caregiver, are critical factors in maintaining the best possible level of care to achieve and then maintain remission.
Early in this journey, because of personal fear and ignorance about this disease, I reached out to the Philadelphia Multiple Myeloma Networking Group (PMMNG). At the first meeting I felt so welcomed and comfortable to be among fellow myeloma patients and their care givers who were all so willing to share their experiences and provide reassurance that we could safely embark on a lifelong journey to overcome this disease. Some group members have been living with myeloma for 18, 22 and even 27years! I now have many new friends and a community that I know and trust to be able to help me and Stephanie through whatever and wherever this disease will take us.
Coming to accept that I have an incurable disease was no small task. Living with myeloma requires PATIENCE and acquiring patience has made my journey much easier. At first, after each monthly blood draw, until I saw the results indicating that my disease was still stable, I used to have significant anxiety. Is this the month that my numbers will skyrocket? Will there be any treatment effective for me? I have come to learn that, although relapse and rising KFLC numbers are an inevitable reality, there is a constant stream of new drugs available for effective treatment. I have also learned from one of my sons – “Why worry until there is really something to worry about?”
I think it is also beneficial to have defined goals. My first goal after diagnosis was to live to attend my oldest grandchild’s Bar Mitzvah which was 2 years ago. Since then, 2 more grandchildren have celebrated their Bar Mitzvahs. The next celebration will be in June 2022, the Bat Mitzvah of my only granddaughter. After the celebrations of the Bar Mitzvahs of my last two grandsons in 2025 and 2029, I will need to search for a new goal. As I learned several years ago, “I may have myeloma, but myeloma doesn’t have me!!”
Having a wife/partner/caregiver intimately involved in my myeloma journey has not only made the journey easier, but has also brought us closer. Stephanie and I are fortunate to have been able to resume travelling – especially with family members. In August 2022 we will take son, daughter-in-law and their three children to the National Parks at the Grand Canyon, Bryce and Zion, as well as a Navajo guided tour of Monument Valley.
We have truly returned to the original mantra of our relationship – “Shame on you if you don’t enjoy every day!”

about the author
Jennifer Ahlstrom
Myeloma survivor, patient advocate, wife, mom of 6. Believer that patients can contribute to cures by joining HealthTree Cure Hub and joining clinical research. Founder and CEO of HealthTree Foundation.
More on Patient Stories




Trending Articles





Upcoming Events




Get the Latest Multiple Myeloma Updates, Delivered to You.
By subscribing to the HealthTree newsletter, you'll receive the latest research, treatment updates, and expert insights to help you navigate your health.
Together we care.
Together we cure.