ASH 2020: Myeloma Experts Debate Duration of Maintenance Therapy

The topic of Minimal Residual Disease (MRD) is permeating a variety of presentations and conversations this year at ASH. Earlier in the week multiple specialists discussed the practical implications of using MRD in clinical trials to identify appropriate end-points.
What other ways can MRD results guide myeloma treatment? A hot topic question with many myeloma patients is about maintenance therapy. Patients may often wonder, does maintenance therapy need to be continued indefinitely or can it be stopped once MRD negativity is achieved?
Myeloma experts Keith Stewart, MBChB Medical Director Princess Margaret Cancer Centre, and Suzanne Lentzsch, MD, PhD Director Multiple Myeloma and Amyloidosis Service at Columbia University Medical Center were recently assigned sides to debate this hot topic during the Friday symposium of ASH. This debate seems far from over, however research continues to emerge for both sides.
Dr. Stewart: Maintenance Should be Indefinite
Maintenance therapy is:
- administered for a prolonged time
- is convenient
- well tolerated long-term and
- does not prevent the use or reduce the efficacy of future treatments
The objective of maintenance treatment is to eliminate or maintain the absence of minimal residual disease (MRD), reduce the risk of relapse and prolong overall and progression free survival.
Results suggest that maintenance with lenalidomide would meet all of these requirements evidenced by research cited by Dr. Stewart as a 26% reduction in risk of death, representing an estimated two and a half year increase in median survival. (McCarthy PL et al. J.Clin Oncol. 2017; 35:3279).
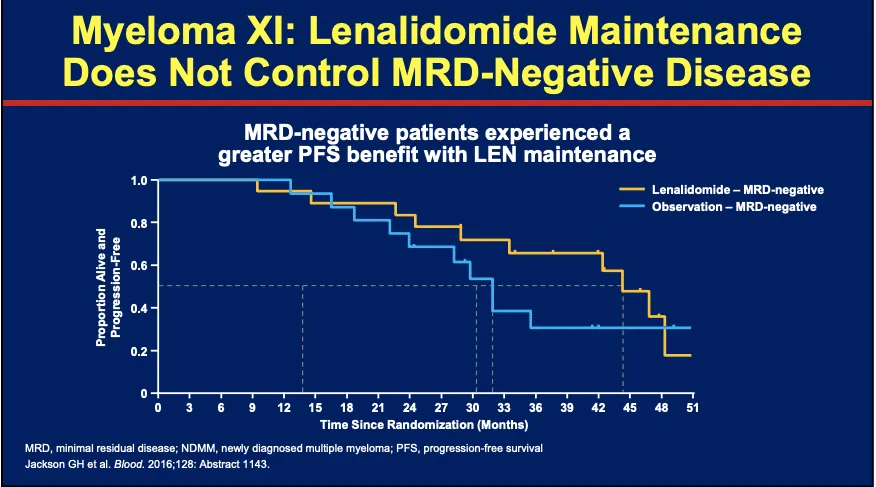
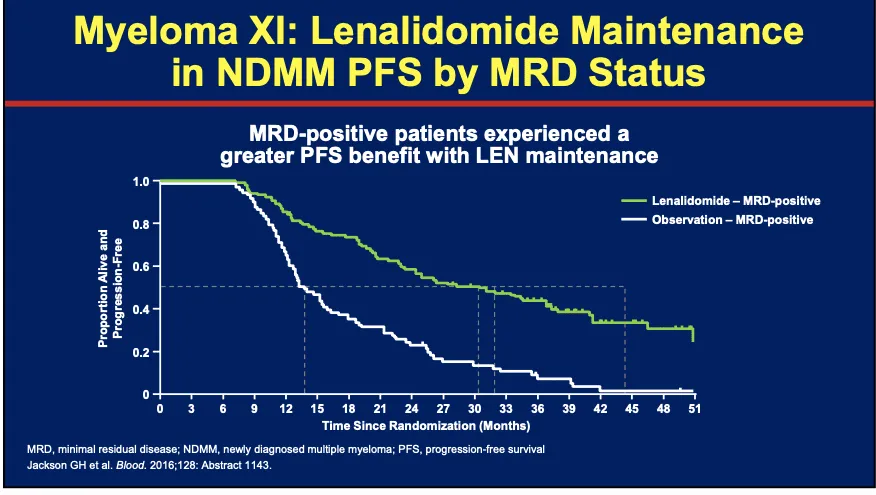
He suggests lenalidomide typically does not impair quality of life, however questions if alone it is sufficient for high risk disease. Research indicates that lenalidomide maintenance does not control MRD negative disease however both MRD negative and MRD positive patients experienced a longer progression free survival (PFS) while on lenalidomide maintenance:
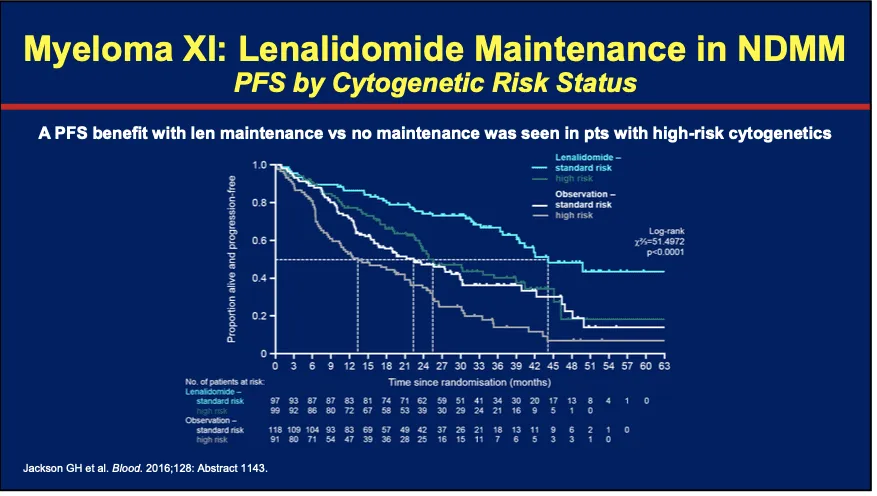
And research does suggest that lenalidomide maintenance vs. observation alone does increase progression free survival for individuals with high risk cytogenetics:
Dr. Lentzsch: Maintenance Should Stop After sustained MRD Negativity is Achieved
Dr. Lentzsch was quick to begin her presentation clarifying that it is well defined that all myeloma patients should receive some form of maintenance therapy. There is no debate that individuals with high risk disease need intensive maintenance.
Currently there is no clinical data to support either continuing or stopping maintenance therapy. However, could minimal residual disease monitoring be used to guide decision making and justify stopping treatment?
The research provided by Dr. Stewart indicates the benefit for maintenance therapy, however is there a sub group of patients who are in complete response who might not need continued maintenance and are being over-treated? Over treating standard risk patients could lead to: decreased quality of life, increased risk of secondary malignancies (such as skin cancer), increased cost and unnecessary side effects such s neutropenia and possible stem cell exhaustion.
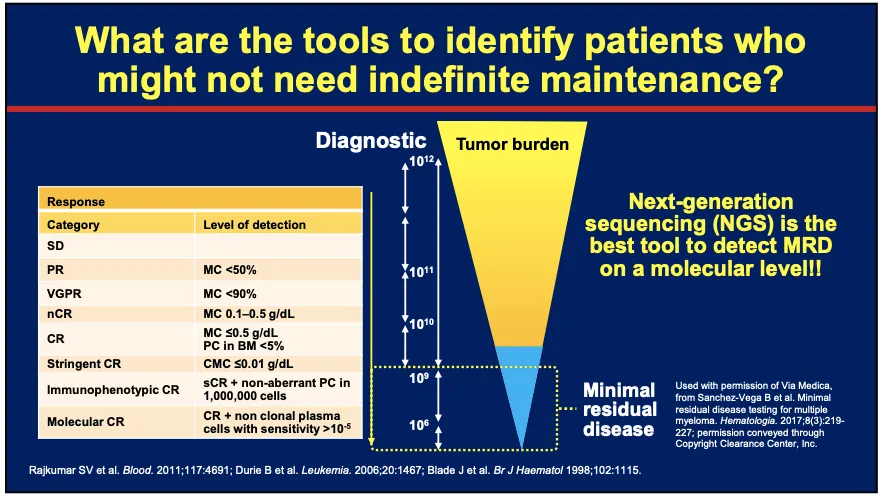
The development of Next Generation Sequencing for minimal residual disease detection at the molecular level is deepening the level of sensitivity to 10-6. Sustained minimal residual disease negativity at this level could begin to guide decision making.
The IFM-DCFI 2009 Study found that measuring minimal residual disease with a sensitive technique like Next Generation Sequencing is highly predictive of progression free survival for patients treated with modern approaches.
Further research indicates that minimal residual disease negativity at the 10-6 sensitivity is needed to identify low risk patients and that the trend can be predictive after three or more measurements.
Dr. Lentszch suggests the information gained from serial MRD testing could help:
- predict clinical risk of progression and prognosis
- Identify patients with low risk of progression (those who are MRD negative using NGS combined with a PET-CT/MRI could be in a molecular remission)
- Identify patients who could consider stopping maintenance. These are individuals who have remained MRD negative over a 3 year period.
- Consider re-starting maintenance if you become MRD positive
No matter which side of the debate you are on, you can use the research shared here to have informed conversations with your myeloma specialist to determine what is best for you.
The Myeloma Crowd recently hosted an interactive webcast on minimal residual disease discussing ways patients can interpret the results. You can view the webcast here.
The topic of Minimal Residual Disease (MRD) is permeating a variety of presentations and conversations this year at ASH. Earlier in the week multiple specialists discussed the practical implications of using MRD in clinical trials to identify appropriate end-points.
What other ways can MRD results guide myeloma treatment? A hot topic question with many myeloma patients is about maintenance therapy. Patients may often wonder, does maintenance therapy need to be continued indefinitely or can it be stopped once MRD negativity is achieved?
Myeloma experts Keith Stewart, MBChB Medical Director Princess Margaret Cancer Centre, and Suzanne Lentzsch, MD, PhD Director Multiple Myeloma and Amyloidosis Service at Columbia University Medical Center were recently assigned sides to debate this hot topic during the Friday symposium of ASH. This debate seems far from over, however research continues to emerge for both sides.
Dr. Stewart: Maintenance Should be Indefinite
Maintenance therapy is:
- administered for a prolonged time
- is convenient
- well tolerated long-term and
- does not prevent the use or reduce the efficacy of future treatments
The objective of maintenance treatment is to eliminate or maintain the absence of minimal residual disease (MRD), reduce the risk of relapse and prolong overall and progression free survival.
Results suggest that maintenance with lenalidomide would meet all of these requirements evidenced by research cited by Dr. Stewart as a 26% reduction in risk of death, representing an estimated two and a half year increase in median survival. (McCarthy PL et al. J.Clin Oncol. 2017; 35:3279).
He suggests lenalidomide typically does not impair quality of life, however questions if alone it is sufficient for high risk disease. Research indicates that lenalidomide maintenance does not control MRD negative disease however both MRD negative and MRD positive patients experienced a longer progression free survival (PFS) while on lenalidomide maintenance:
And research does suggest that lenalidomide maintenance vs. observation alone does increase progression free survival for individuals with high risk cytogenetics:
Dr. Lentzsch: Maintenance Should Stop After sustained MRD Negativity is Achieved
Dr. Lentzsch was quick to begin her presentation clarifying that it is well defined that all myeloma patients should receive some form of maintenance therapy. There is no debate that individuals with high risk disease need intensive maintenance.
Currently there is no clinical data to support either continuing or stopping maintenance therapy. However, could minimal residual disease monitoring be used to guide decision making and justify stopping treatment?
The research provided by Dr. Stewart indicates the benefit for maintenance therapy, however is there a sub group of patients who are in complete response who might not need continued maintenance and are being over-treated? Over treating standard risk patients could lead to: decreased quality of life, increased risk of secondary malignancies (such as skin cancer), increased cost and unnecessary side effects such s neutropenia and possible stem cell exhaustion.
The development of Next Generation Sequencing for minimal residual disease detection at the molecular level is deepening the level of sensitivity to 10-6. Sustained minimal residual disease negativity at this level could begin to guide decision making.
The IFM-DCFI 2009 Study found that measuring minimal residual disease with a sensitive technique like Next Generation Sequencing is highly predictive of progression free survival for patients treated with modern approaches.
Further research indicates that minimal residual disease negativity at the 10-6 sensitivity is needed to identify low risk patients and that the trend can be predictive after three or more measurements.
Dr. Lentszch suggests the information gained from serial MRD testing could help:
- predict clinical risk of progression and prognosis
- Identify patients with low risk of progression (those who are MRD negative using NGS combined with a PET-CT/MRI could be in a molecular remission)
- Identify patients who could consider stopping maintenance. These are individuals who have remained MRD negative over a 3 year period.
- Consider re-starting maintenance if you become MRD positive
No matter which side of the debate you are on, you can use the research shared here to have informed conversations with your myeloma specialist to determine what is best for you.
The Myeloma Crowd recently hosted an interactive webcast on minimal residual disease discussing ways patients can interpret the results. You can view the webcast here.

about the author
Rozalynn Hite
Rozalynn Hite is the HealthTree Coach Director and wife of myeloma patient Richard Hite. Rozalynn is an occupational therapist and mother of three beautiful children. She is passionate about providing support, education, and resources to help others live full and active lives.
More on Conferences






Trending Articles



Upcoming Events




Get the Latest Multiple Myeloma Updates, Delivered to You.
By subscribing to the HealthTree newsletter, you'll receive the latest research, treatment updates, and expert insights to help you navigate your health.
Together we care.
Together we cure.