ASH 2020: High Risk Smoldering Myeloma-Is It Time To Treat?

The debate over when and how to treat high risk smoldering multiple myeloma patients (HRSMM) has heated up again at this year's ASH conference. HRSMM is defined as having at least a 50% chance of progressing to active myeloma within 2 years and 75% in 5 years. We'll review the basis of the current definition and recommendations, as well as several studies that are bringing us closer to finding more exacting individual genomic and immune parameters upon which to base the definition.
Based on the discussions below, we come to three important conclusions:
- Many high risk genetic factors are developed in the precursor stage, so if they exist and we know they will become aggressive myeloma, why not treat earlier for those patients?
- New blood tests could tell how strong our immune systems would be at keeping active myeloma at bay
- Precursor conditions could be prevented from progressing with early immunotherapy use
In a session "When Should High Risk Smoldering Be Treated?" led by Dr. Shaji Kumar along with seven other members of the International Myeloma Working (IMWG) group, they made the case for their conclusion that we have adequate evidence to recommend that HRSMM patients either receive treatment with lenalidomide only or add dexamethasone, or join clinical trials. This is captured in a proposed algorithm for 2021 by Dr. Vincent Rajkumar on behalf of the International Myeloma Working Group.
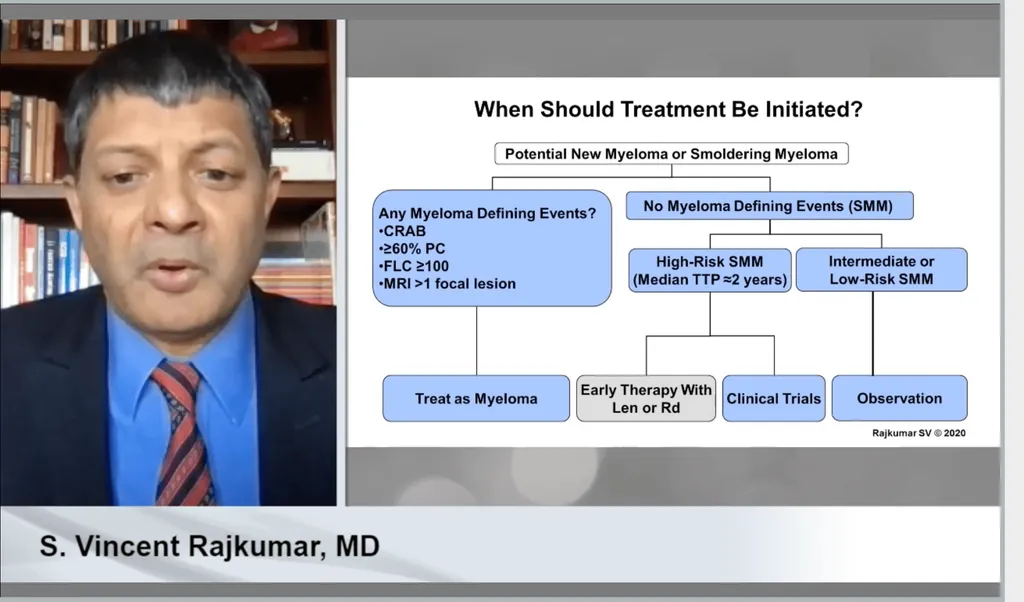
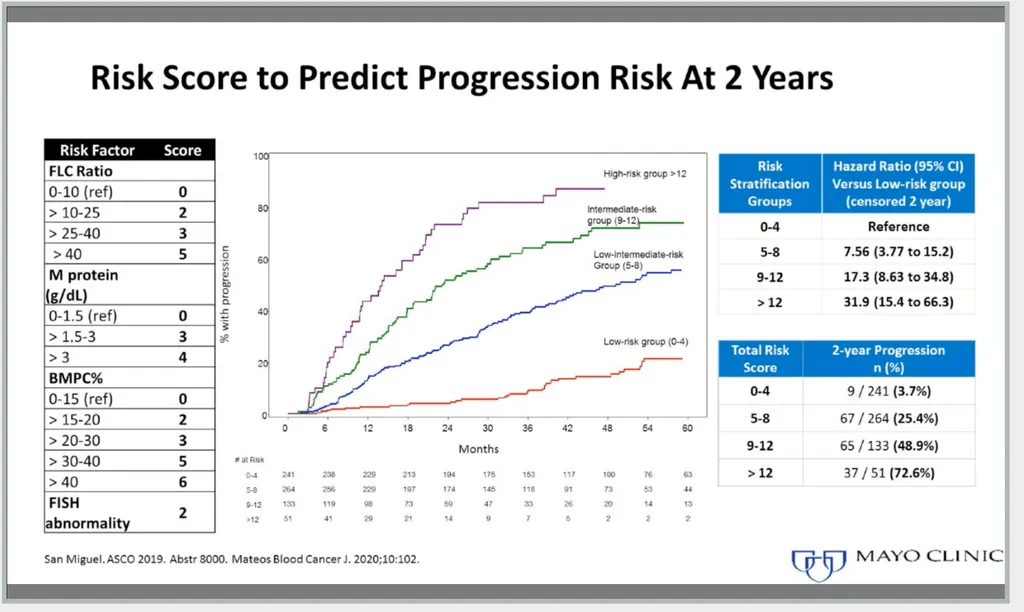
Evidence used to support this recommendation include the updated IMWG 2/20/20 criteria: >2 grams/deciliter of serum M-protein, >20% serum free light-chain ratio, and >20% plasma cells found by bone marrow biopsy. An IMWG Risk Score Tool was also developed which offers the incorporation of cytogenetics.
Important additional evidence comes from three studies:
- 1. The first is the 11 year readout of the Phase 3 Spanish QuiReDex trial that compared treatment with lenalidomide (Revlimid) and dexamethasone vs. observation has shown an overall survival benefit of 6.4 yrs lenalidomide/dexamethasone vs 4.7 yrs with observation. It also shows a progression free survival benefit for treatment. Unfortunately patients were not screened with imaging in order to qualify so some may have actually had active myeloma, therefore many specialists do not accept any results from this trial as evidence for the benefit of early treatment.
- The second are the recent results of the Phase 3 ECOG study, EA306, lenalidomide only vs observation in both high risk and intermediate risk smoldering myeloma patients which showed at a 35 month readout a 3 year progression free survival benefit of 91% vs 66% for the lenalidomide vs observation arms. The conclusion from this trial is that early treatment of high risk smoldering myeloma patients delays symptomatic progression and the risk of end organ damage.
- At ASH Dr. Dickran Kazandjian of the National Institutes of Health (NIH), reported results of a study to treat high risk smoldering myeloma patients with carfilzomib (Kyprolis ® or K), Revlimid and dexamethasone (KRd) with Revlimid maintenance. A total of 52 patients were enrolled with the goal of preventing the onset of active myeloma. 10% of patients developed active myeloma versus historical rates with no treatment of ~75%. 100% of the study participants were alive and had an overall response. A minimal residual disease negative (MRD-) response for more than 5.5 years was achieved by 39.3%, and 77.5% had a 24-month sustained response.
This evidence shows an increase in progression free survival and a questionable increase in overall survival for early treatment. However, there are specialists who prefer to wait for genomic, kinetic and immune biomarkers that no longer assume "the disease" progresses in a linear manner, or even is one disease and will provide individualized data regarding risk of progression, before recommending early treatment which is accompanied by toxicities.
Here are three of the research studies on high risk smoldering myeloma I find incredibly exciting and for each I'll share why.
- Abstract #602: WHOLE-GENOME SEQUENCING REVEALS EVIDENCE OF TWO BIOLOGICLLY AND CLINICALLY DISTICT ENTITIES: PROGRESSIVE VERSUS STABLE MYELOMA PRECURSOR DISEASE https://ash.confex.com/ash/2020/webprogram/Paper136403.html
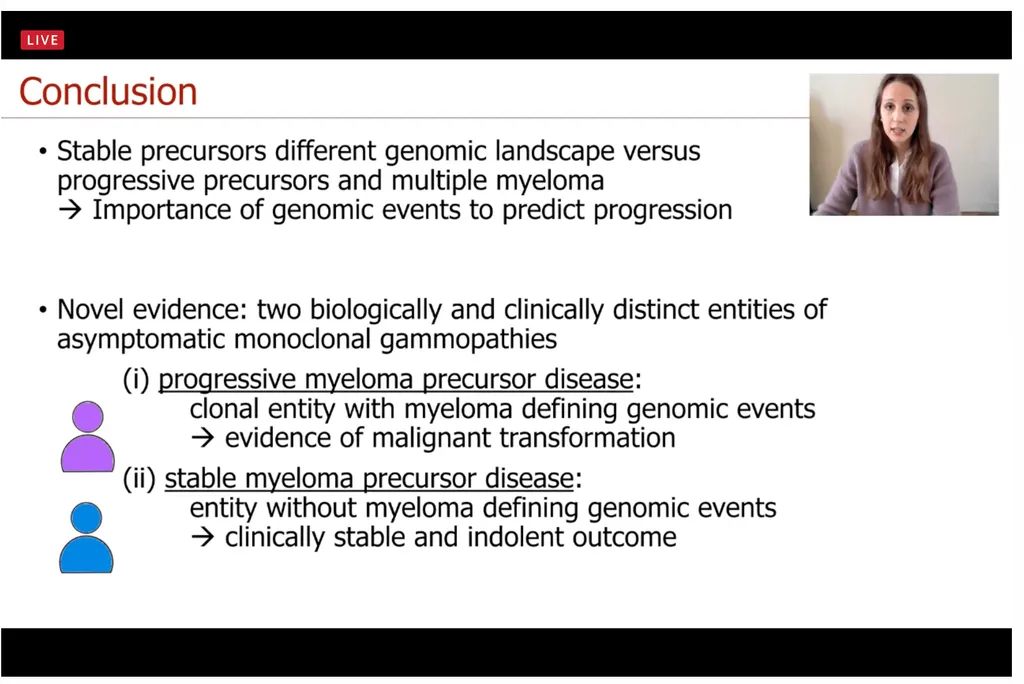
Dr. Benedith Oben of Belgium presented the first whole-genome sequencing (WGS) analysis of patients with monoclonal gammopathy of unknown significance (MGUS) and smoldering multiple myeloma (SMM) wherein they successfully identified two distinct mutational landscapes for stable precursors and progressive precursors.
Bone marrow samples of a total of 32 patients, 18 MGUS and 14 SMM were analyzed and compared to 80 myeloma patients with the following findings.
Key findings:
- At 40.5 months 15 of 32 patients were stable and 17 progressed.
- Progressive precursors- most genomic drivers already acquired (earlier in life) conferring high risk of progression
- Stable precursors - acquire multi-gain events later in life which do not harbor key genomic MM hallmarks
- Cytogenetics - no differences found between progressive myeloma precursor cases and multiple myeloma
- Stable precursors- lower incidence of Structural Variants and Complex events
- Progressive precursors - 85% had APOBEC mutational activity
Here are Dr. Oben's conclusions:
- Abstract #57: Longitudinal Profiling of Tumor and Immune Cells for Minimally-Invasive Monitoring of Smoldering Multiple Myeloma (SMM): The Immunocell Study. https://ash.confex.com/ash/2020/webprogram/Paper136251.html
Dr. Rosalinda Termini of University Clinic of Navarra, Pamplona, Spain who presented, said "New minimally-invasive methods should also monitor immune profiles, to identify patients with stable tumor/burden genetics but at risk of progression due to lost immune surveillance."
This research says it's not just about how aggressive or not the clones are, but about how well our immune systems monitor and respond to our abnormal plasma cells!
I love the topline goal of this trial which is to eventually use peripheral blood samples taken in the clinic to evaluate Circulating Tumor Cells (CTCs) and immune subsets to identify if you are at risk of progression to active disease.
Importantly, at interim analysis 8 of 18 patients who had progressive disease were not high risk smoldering myeloma (SMM) by the 20/2/20 model. Dr. Termini said they think Immunocell technology can be used to enhance the 20/2/20 model.
Specific aims were to:
- compare immune profiles from SMM vs healthy individuals and MM patients
- define immune signatures in SMM related to disease stability vs progression.
- compare data with current stratification models that are based on serological and bone marrow (BM) assessments.
- look at the concordance between the tumor/immune landscape of the bone marrow vs peripheral blood of SMM patients (so eventually we can only use non-invasive blood samples)
- evaluate immune subsets together with Circulating Tumor Cells (CTCs) using single-cell technology
- evaluate clonal heterogeneity over time
- generate knowledge on pathogenesis and dissemination of SMM to active MM
- generate large datasets on CTTC-RNAseq, AATAseq and immunoscores from SMM pts
- develop minimally-invasive algorithms to tailor pre-emptive immunotherapies
Methods and Study design:
- At time of conference 170 patients enrolled, 150 reported on of accrual goal 300 patients
- Peripheral blood samples every 6 months were mandatory with bone marrow samples optional
- Absolute CTCs determined by next-generation flow cytometry
- Immune profiling using multidimensional flow cytometry and semi-automated data analysis
- Next-generation flow (NGF) for monitoring of CTCs and immune profiles
- Flow-sorting of tumor cells and three immune effector cell types in each sample
Her conclusions can be seen here.
- Abstract #485: Extensive Changes of the Immune Microenvironment Are Associated with Progression from Precursor Stages to Multiple Myeloma. https://ash.confex.com/ash/2020/webprogram/Paper137555.html
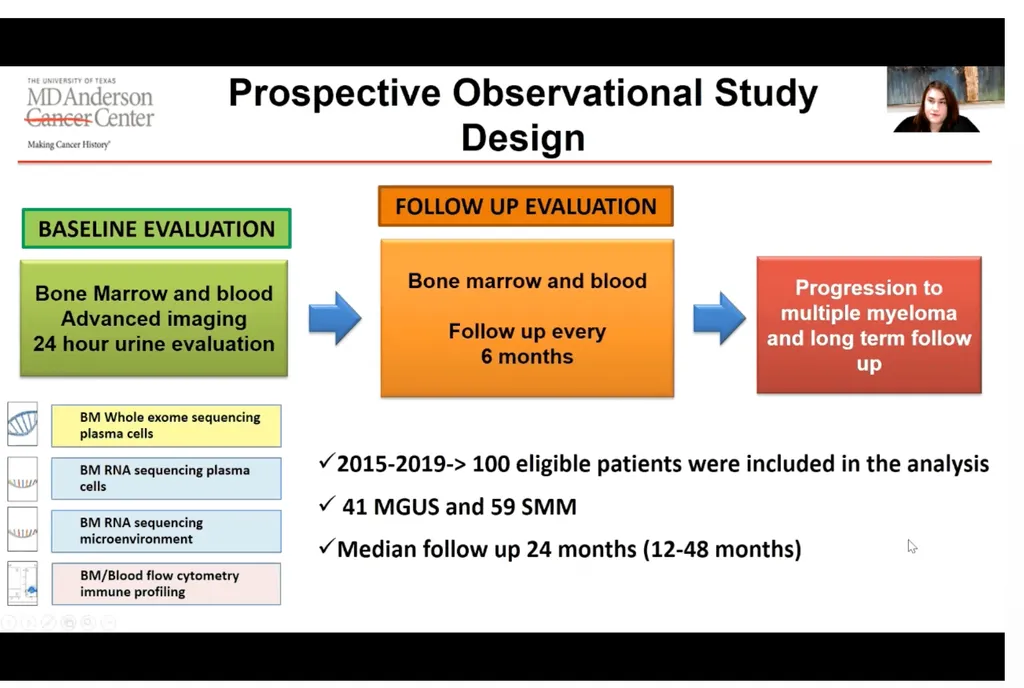
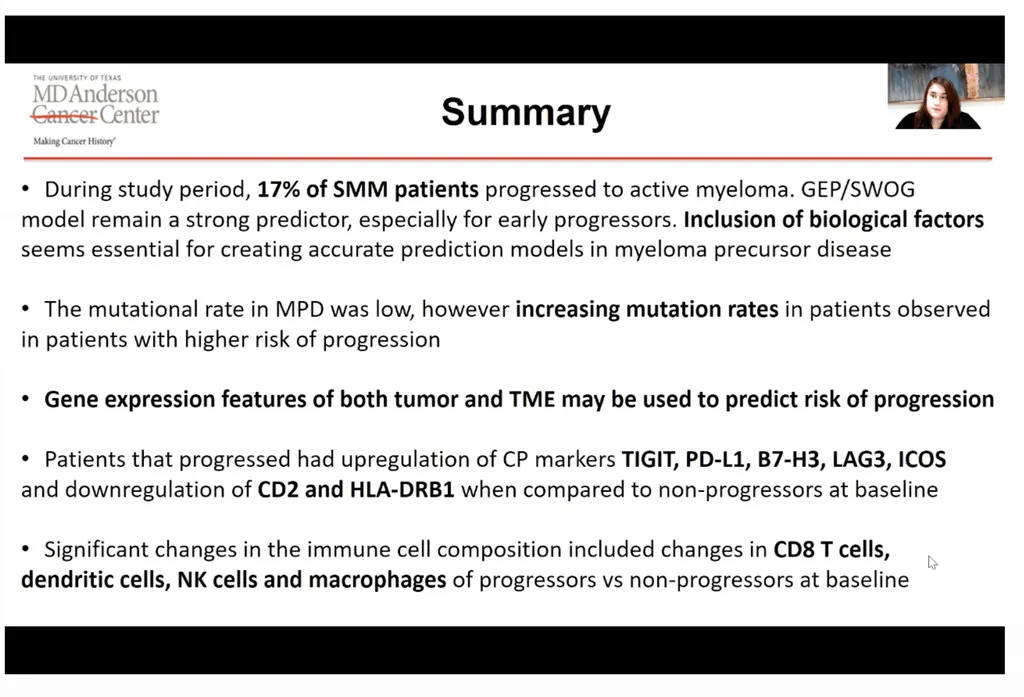
Dr. Elisabet Manasanch of MD Anderson presented a third research study we should keep on our radar. What excites me most here is that she believes this research provides a rationale to halt progression of the disease with immunotherapy.
The basis for this research is that it is known that as early as MGUS, changes take place in immune cells and their function that result in reduced tumor surveillance.
The primary aims were to:
- characterize immune dysregulation in myeloma precursor disease
- describe changes in the evolution to active multiple myeloma
These slides capture the study design and conclusions.
Having reviewed the "what we know" and the "what we've yet to learn", my hope is that if you are a high risk smoldering myeloma patient making a treatment decision going into 2021, you will be introspective regarding your medical risk tolerance and combine this with thoughtful discussion with your myeloma specialist regarding the known details of your individual disease behavior and biology.
You will also need to select a specialist who has a treatment philosophy that aligns with your own. I truly believe knowledge is power, so please keep reading and learning.
The debate over when and how to treat high risk smoldering multiple myeloma patients (HRSMM) has heated up again at this year's ASH conference. HRSMM is defined as having at least a 50% chance of progressing to active myeloma within 2 years and 75% in 5 years. We'll review the basis of the current definition and recommendations, as well as several studies that are bringing us closer to finding more exacting individual genomic and immune parameters upon which to base the definition.
Based on the discussions below, we come to three important conclusions:
- Many high risk genetic factors are developed in the precursor stage, so if they exist and we know they will become aggressive myeloma, why not treat earlier for those patients?
- New blood tests could tell how strong our immune systems would be at keeping active myeloma at bay
- Precursor conditions could be prevented from progressing with early immunotherapy use
In a session "When Should High Risk Smoldering Be Treated?" led by Dr. Shaji Kumar along with seven other members of the International Myeloma Working (IMWG) group, they made the case for their conclusion that we have adequate evidence to recommend that HRSMM patients either receive treatment with lenalidomide only or add dexamethasone, or join clinical trials. This is captured in a proposed algorithm for 2021 by Dr. Vincent Rajkumar on behalf of the International Myeloma Working Group.
Evidence used to support this recommendation include the updated IMWG 2/20/20 criteria: >2 grams/deciliter of serum M-protein, >20% serum free light-chain ratio, and >20% plasma cells found by bone marrow biopsy. An IMWG Risk Score Tool was also developed which offers the incorporation of cytogenetics.
Important additional evidence comes from three studies:
- 1. The first is the 11 year readout of the Phase 3 Spanish QuiReDex trial that compared treatment with lenalidomide (Revlimid) and dexamethasone vs. observation has shown an overall survival benefit of 6.4 yrs lenalidomide/dexamethasone vs 4.7 yrs with observation. It also shows a progression free survival benefit for treatment. Unfortunately patients were not screened with imaging in order to qualify so some may have actually had active myeloma, therefore many specialists do not accept any results from this trial as evidence for the benefit of early treatment.
- The second are the recent results of the Phase 3 ECOG study, EA306, lenalidomide only vs observation in both high risk and intermediate risk smoldering myeloma patients which showed at a 35 month readout a 3 year progression free survival benefit of 91% vs 66% for the lenalidomide vs observation arms. The conclusion from this trial is that early treatment of high risk smoldering myeloma patients delays symptomatic progression and the risk of end organ damage.
- At ASH Dr. Dickran Kazandjian of the National Institutes of Health (NIH), reported results of a study to treat high risk smoldering myeloma patients with carfilzomib (Kyprolis ® or K), Revlimid and dexamethasone (KRd) with Revlimid maintenance. A total of 52 patients were enrolled with the goal of preventing the onset of active myeloma. 10% of patients developed active myeloma versus historical rates with no treatment of ~75%. 100% of the study participants were alive and had an overall response. A minimal residual disease negative (MRD-) response for more than 5.5 years was achieved by 39.3%, and 77.5% had a 24-month sustained response.
This evidence shows an increase in progression free survival and a questionable increase in overall survival for early treatment. However, there are specialists who prefer to wait for genomic, kinetic and immune biomarkers that no longer assume "the disease" progresses in a linear manner, or even is one disease and will provide individualized data regarding risk of progression, before recommending early treatment which is accompanied by toxicities.
Here are three of the research studies on high risk smoldering myeloma I find incredibly exciting and for each I'll share why.
- Abstract #602: WHOLE-GENOME SEQUENCING REVEALS EVIDENCE OF TWO BIOLOGICLLY AND CLINICALLY DISTICT ENTITIES: PROGRESSIVE VERSUS STABLE MYELOMA PRECURSOR DISEASE https://ash.confex.com/ash/2020/webprogram/Paper136403.html
Dr. Benedith Oben of Belgium presented the first whole-genome sequencing (WGS) analysis of patients with monoclonal gammopathy of unknown significance (MGUS) and smoldering multiple myeloma (SMM) wherein they successfully identified two distinct mutational landscapes for stable precursors and progressive precursors.
Bone marrow samples of a total of 32 patients, 18 MGUS and 14 SMM were analyzed and compared to 80 myeloma patients with the following findings.
Key findings:
- At 40.5 months 15 of 32 patients were stable and 17 progressed.
- Progressive precursors- most genomic drivers already acquired (earlier in life) conferring high risk of progression
- Stable precursors - acquire multi-gain events later in life which do not harbor key genomic MM hallmarks
- Cytogenetics - no differences found between progressive myeloma precursor cases and multiple myeloma
- Stable precursors- lower incidence of Structural Variants and Complex events
- Progressive precursors - 85% had APOBEC mutational activity
Here are Dr. Oben's conclusions:
- Abstract #57: Longitudinal Profiling of Tumor and Immune Cells for Minimally-Invasive Monitoring of Smoldering Multiple Myeloma (SMM): The Immunocell Study. https://ash.confex.com/ash/2020/webprogram/Paper136251.html
Dr. Rosalinda Termini of University Clinic of Navarra, Pamplona, Spain who presented, said "New minimally-invasive methods should also monitor immune profiles, to identify patients with stable tumor/burden genetics but at risk of progression due to lost immune surveillance."
This research says it's not just about how aggressive or not the clones are, but about how well our immune systems monitor and respond to our abnormal plasma cells!
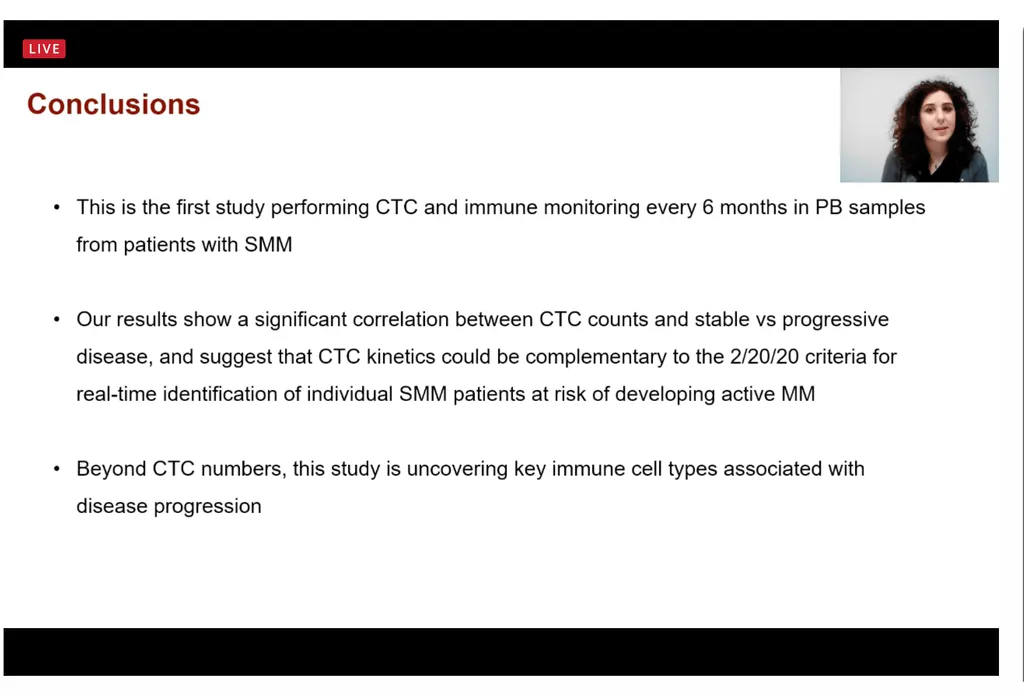
I love the topline goal of this trial which is to eventually use peripheral blood samples taken in the clinic to evaluate Circulating Tumor Cells (CTCs) and immune subsets to identify if you are at risk of progression to active disease.
Importantly, at interim analysis 8 of 18 patients who had progressive disease were not high risk smoldering myeloma (SMM) by the 20/2/20 model. Dr. Termini said they think Immunocell technology can be used to enhance the 20/2/20 model.
Specific aims were to:
- compare immune profiles from SMM vs healthy individuals and MM patients
- define immune signatures in SMM related to disease stability vs progression.
- compare data with current stratification models that are based on serological and bone marrow (BM) assessments.
- look at the concordance between the tumor/immune landscape of the bone marrow vs peripheral blood of SMM patients (so eventually we can only use non-invasive blood samples)
- evaluate immune subsets together with Circulating Tumor Cells (CTCs) using single-cell technology
- evaluate clonal heterogeneity over time
- generate knowledge on pathogenesis and dissemination of SMM to active MM
- generate large datasets on CTTC-RNAseq, AATAseq and immunoscores from SMM pts
- develop minimally-invasive algorithms to tailor pre-emptive immunotherapies
Methods and Study design:
- At time of conference 170 patients enrolled, 150 reported on of accrual goal 300 patients
- Peripheral blood samples every 6 months were mandatory with bone marrow samples optional
- Absolute CTCs determined by next-generation flow cytometry
- Immune profiling using multidimensional flow cytometry and semi-automated data analysis
- Next-generation flow (NGF) for monitoring of CTCs and immune profiles
- Flow-sorting of tumor cells and three immune effector cell types in each sample
Her conclusions can be seen here.
- Abstract #485: Extensive Changes of the Immune Microenvironment Are Associated with Progression from Precursor Stages to Multiple Myeloma. https://ash.confex.com/ash/2020/webprogram/Paper137555.html
Dr. Elisabet Manasanch of MD Anderson presented a third research study we should keep on our radar. What excites me most here is that she believes this research provides a rationale to halt progression of the disease with immunotherapy.
The basis for this research is that it is known that as early as MGUS, changes take place in immune cells and their function that result in reduced tumor surveillance.
The primary aims were to:
- characterize immune dysregulation in myeloma precursor disease
- describe changes in the evolution to active multiple myeloma
These slides capture the study design and conclusions.
Having reviewed the "what we know" and the "what we've yet to learn", my hope is that if you are a high risk smoldering myeloma patient making a treatment decision going into 2021, you will be introspective regarding your medical risk tolerance and combine this with thoughtful discussion with your myeloma specialist regarding the known details of your individual disease behavior and biology.
You will also need to select a specialist who has a treatment philosophy that aligns with your own. I truly believe knowledge is power, so please keep reading and learning.

about the author
Bonnie Falbo
Bonnie is a Myeloma Coach and the caregiver for her husband with Multiple Myeloma. They live at the foot of the Blue Ridge Mountains in Afton, VA with their 2 dogs and 2 cats.
More on Conferences






Trending Articles



Upcoming Events


Get the Latest Multiple Myeloma Updates, Delivered to You.
By subscribing to the HealthTree newsletter, you'll receive the latest research, treatment updates, and expert insights to help you navigate your health.
Together we care.
Together we cure.