ASH 2022: Improved Quality of Life on Quad Therapy

As patients, we’re always concerned if our oncologist suggests adding yet another drug to a regimen that already seems onerous. The addition of another drug may result in a better treatment outcome, but at what cost to our own health and well-being?
Recent data shows that adding daratumamab to the standard of care regimen following transplant results in improved patient outcomes as well as improved quality of life for patients. Patients actually felt better with the additional chemotherapeutic agent.
The well accepted standard of care for newly diagnosed transplant-eligible multiple myeloma patients is induction with bortezamib, lenalidamide, and dexamethazone (VRd) followed by transplant and then consolidation with VRd and maintenance with lenalidamide alone. The GRIFFIN study looked at the addition of daratumamab (D-VRd) to each one of the chemotherapeutic phases. The data showed a deepening, prolonged response with the D-VRd regimen compared to VRd. However, at what cost to the patient’s quality of life?
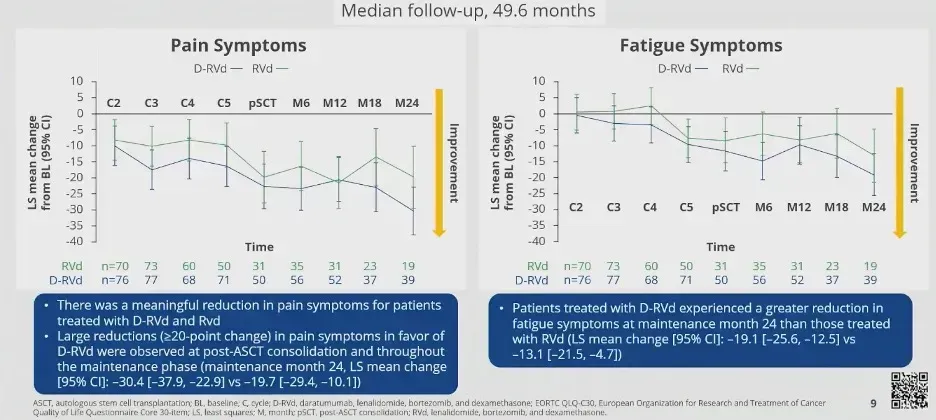
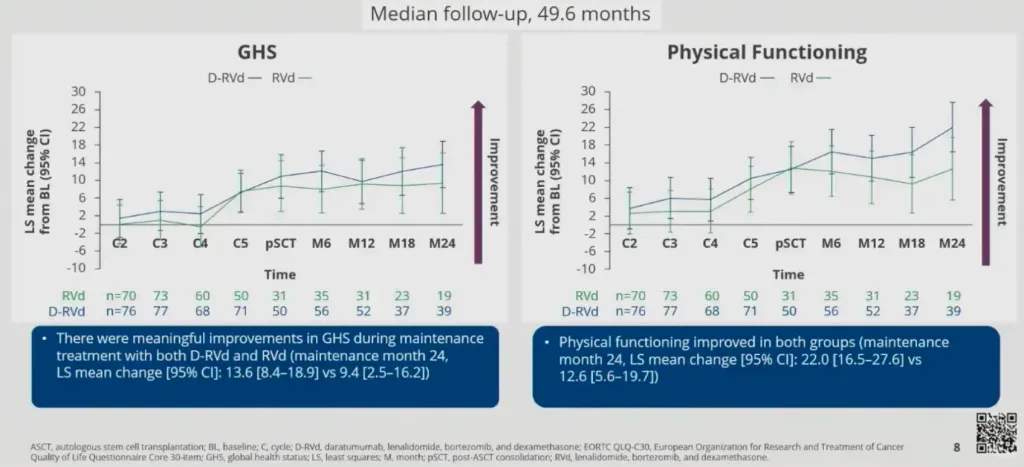
One group looked at the patients in the GRIFFIN study with a focus on patient-reported quality of life. These data points included global health status, physical functionality, pain, and fatigue. Patients in both arms of the study reported improvement in all of these areas, with a greater degree of improvement reported by those who received daratumamab as part of their treatment regimen.
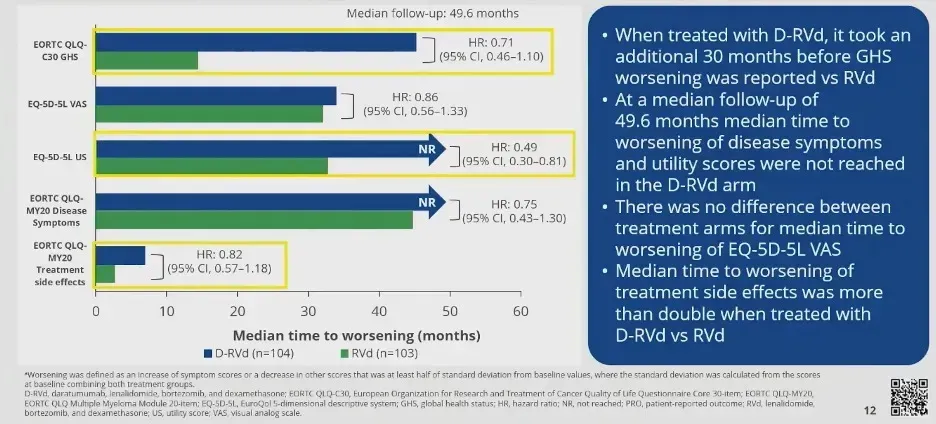
Additionally, the patient reported worsening of disease symptoms was significantly sooner with the group of patients receiving RVd alone.
Interestingly, this is despite daratumamab being administered IV. One might postulate that the results would be even more dramatic utilizing the even more convenient subcutaneous Darzalex FASPRO.
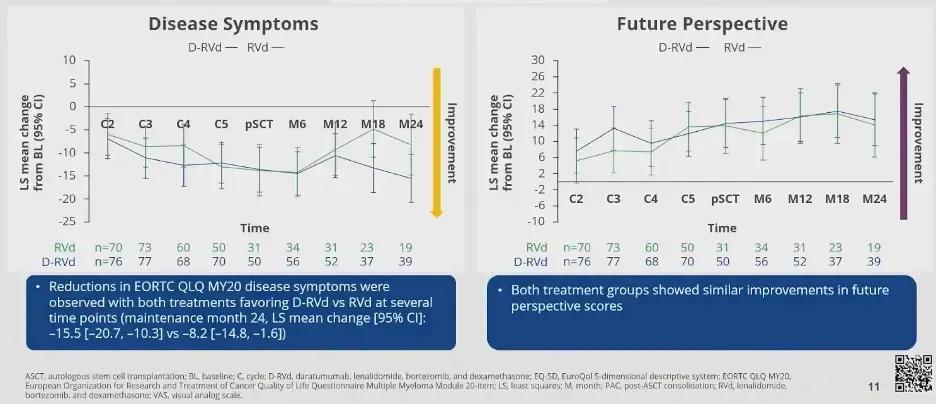
Disease symptoms and the patient’s future perspectives also improved in both arms, with the daratumamab arm showing more significant improvements than the standard of care arm. This is despite an increased rate of cytopenia and infection with the addition of daratumamab.
We would naturally anticipate a decrease in our quality of life with each new agent that is added to our chemotherapeutic regimen. However, this data sets that notion on its ear by showing that a patient’s quality of life improves with the addition of daratumamab, an agent which has also demonstrated a deepening of response and increased progression-free survival when added to the standard of care regimen.
It seems counterintuitive that the quality of life can improve with more chemotherapeutic agents, but this important patient-reported outcome study provides strong support for increasing quality of life by doing just that.
As patients, we’re always concerned if our oncologist suggests adding yet another drug to a regimen that already seems onerous. The addition of another drug may result in a better treatment outcome, but at what cost to our own health and well-being?
Recent data shows that adding daratumamab to the standard of care regimen following transplant results in improved patient outcomes as well as improved quality of life for patients. Patients actually felt better with the additional chemotherapeutic agent.
The well accepted standard of care for newly diagnosed transplant-eligible multiple myeloma patients is induction with bortezamib, lenalidamide, and dexamethazone (VRd) followed by transplant and then consolidation with VRd and maintenance with lenalidamide alone. The GRIFFIN study looked at the addition of daratumamab (D-VRd) to each one of the chemotherapeutic phases. The data showed a deepening, prolonged response with the D-VRd regimen compared to VRd. However, at what cost to the patient’s quality of life?
One group looked at the patients in the GRIFFIN study with a focus on patient-reported quality of life. These data points included global health status, physical functionality, pain, and fatigue. Patients in both arms of the study reported improvement in all of these areas, with a greater degree of improvement reported by those who received daratumamab as part of their treatment regimen.
Additionally, the patient reported worsening of disease symptoms was significantly sooner with the group of patients receiving RVd alone.
Interestingly, this is despite daratumamab being administered IV. One might postulate that the results would be even more dramatic utilizing the even more convenient subcutaneous Darzalex FASPRO.
Disease symptoms and the patient’s future perspectives also improved in both arms, with the daratumamab arm showing more significant improvements than the standard of care arm. This is despite an increased rate of cytopenia and infection with the addition of daratumamab.
We would naturally anticipate a decrease in our quality of life with each new agent that is added to our chemotherapeutic regimen. However, this data sets that notion on its ear by showing that a patient’s quality of life improves with the addition of daratumamab, an agent which has also demonstrated a deepening of response and increased progression-free survival when added to the standard of care regimen.
It seems counterintuitive that the quality of life can improve with more chemotherapeutic agents, but this important patient-reported outcome study provides strong support for increasing quality of life by doing just that.

about the author
Kyle Colvin, MD
“As a physician, I figured I may have a unique perspective on the disease, as well as a knowledge base and the time to help patients understand the disease course and treatment options. I figure that I should give back to those in need since my life has been incredibly fortunate, even with this disease.”
More on Conferences















Get the Latest Multiple Myeloma Updates, Delivered to You.
By subscribing to the HealthTree newsletter, you'll receive the latest research, treatment updates, and expert insights to help you navigate your health.
Together we care.
Together we cure.