How Myeloma Induction Therapy Is Evolving: Vital Insights for Newly Diagnosed Patients

Dr. Francecsa Gay presented important data surrounding multiple myeloma induction therapy at the International Myeloma Society (IMS) meeting in Rio de Janeiro, Brazil.
Read on to learn more about the goals of induction therapy, as well as open questions such as optimal treatment cycles and schedules and how to improve induction therapy outcomes for high-risk multiple myeloma.
Goals of Induction Therapy in Multiple Myeloma
The main goals of induction therapy in newly diagnosed multiple myeloma are to control the disease quickly and effectively while keeping side effects manageable. This first phase of treatment is essential to set up the best possible outcomes for what comes next, like a potential stem cell transplant.
The key goals of induction therapy include:
-
Quickly lowering the number of myeloma cells to gain fast control over the disease.
-
Achieving a deep response—ideally, a Very Good Partial Response (VGPR) or better, aiming for MRD negativity (no detectable myeloma cells).
-
Making sure treatment is well-tolerated, with minimal side effects.
Preparing for a successful stem cell harvest for patients who may be eligible for a stem cell transplant.
Achieving Deep Responses to Myeloma Therapy
Newly diagnosed myeloma patients can often achieve strong responses to induction therapy. The chart below highlights the average response levels patients can expect after completing their induction treatments.

Today’s myeloma treatment strategies make it possible for many patients to reach a VGPR (Very Good Partial Response) or even higher. Some induction therapies, especially quadruplet (4-drug) combinations, can lead to deep responses in a large portion of patients—often reaching minimal residual disease (MRD) negativity. This means that no myeloma cells are detected in a sample size as large as 100,000 to 1,000,000 cells, depending on the test.
Want to learn more about treatments and therapies for multiple myeloma from experts? Start watching HealthTree University videos here:
Safety in Induction Therapy
Fortunately, most induction therapies for newly diagnosed myeloma patients have a very low rate of discontinuation due to side effects, and treatment-related deaths during this phase are even rarer.
The primary concern for patients during this phase remains the risk of infections. This is due to both the immune system being compromised by myeloma itself and the side effects of treatment. Severe, life-threatening infections are uncommon at this stage.
Collecting Stem Cells: What to Expect
About 95-99% of multiple myeloma patients eligible for a stem cell transplant can successfully collect enough stem cells through a process called apheresis.
If anti-CD38 therapy (like daratumumab or isatuximab) is part of a patient’s four-drug induction therapy, they may collect slightly fewer stem cells than those on a three-drug regimen. However, 95% of patients still gather an adequate amount, so this isn’t typically a major concern.
Are you preparing for a stem cell transplant or curious about the process? Check out our stem cell transplant education guide here:
What’s Next for Myeloma Induction Therapy?
While the data presented above is promising, questions still remain such as:
-
What is the optimal number of treatment cycles for certain combinations? What’s the most efficient treatment schedule to get the best results?
and
-
What more can be done for high-risk myeloma patients whose responses tend to be shorter than those with standard-risk myeloma?
Optimizing Treatment Cycles and Schedules
Myeloma researchers have explored a six-cycle regimen with triplet (3-drug) therapies during induction, which has shown improvements in both response rates and depth, especially in helping patients reach VGPR (Very Good Partial Response). The next goal is to further boost these response rates by using quadruplet (4-drug) induction therapies.
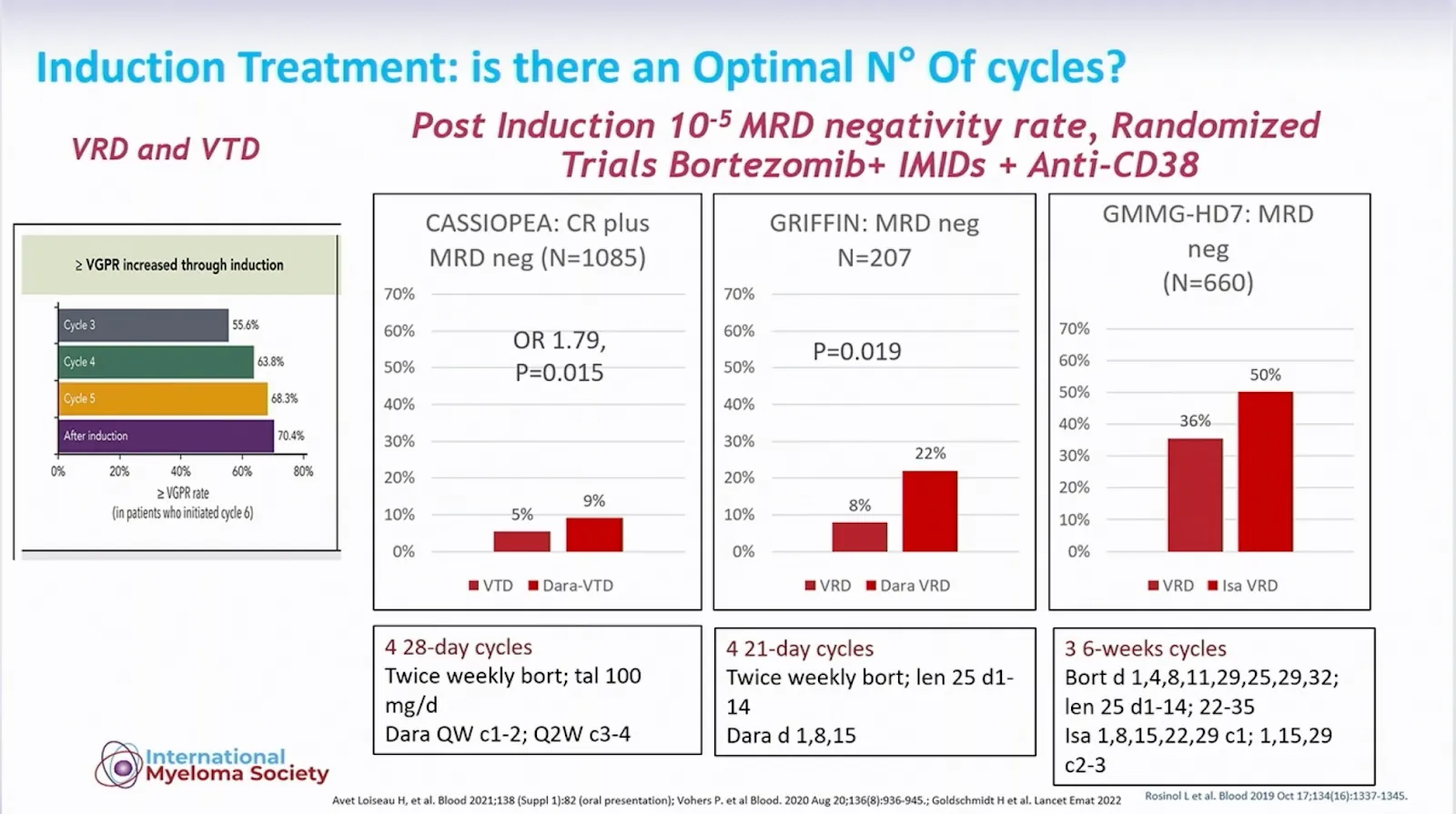
In the recent GMMG-HD7 trial (shown on the right of the image above), a 12-week induction therapy achieved a 50% MRD negativity rate. This is the highest rate of such a deep response seen so far compared to other bortezomib (Velcade)--based quadruplet induction therapies.
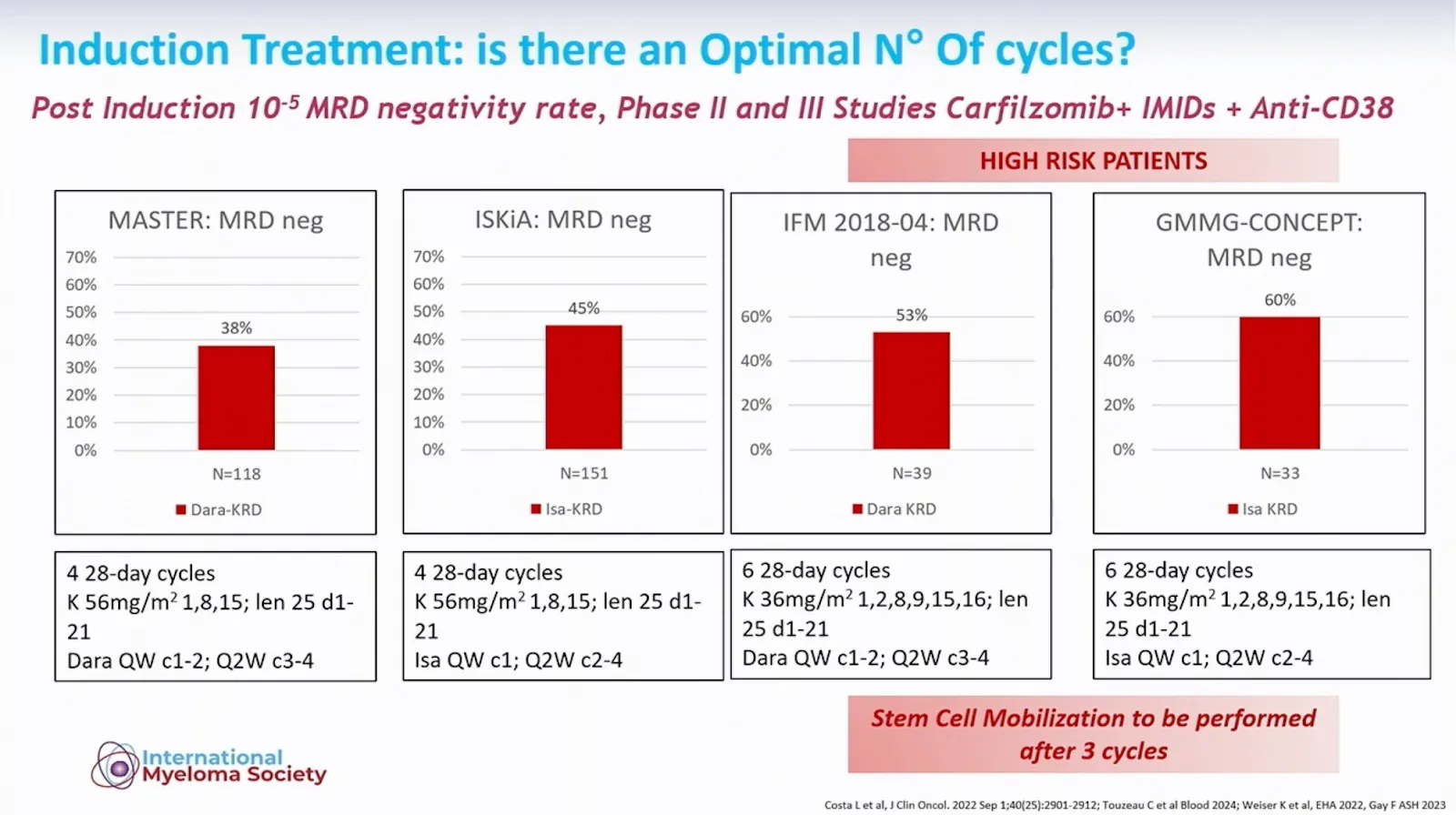
The image above shows MRD-negative rates achieved with carfilzomib (Kyprolis)- based quadruplet induction therapies. Two trials, IFM 2018-04 and GMMG-CONCEPT, focused specifically on high-risk multiple myeloma patients and used an extended induction therapy of six 28-day cycles.
After this extended induction therapy:
-
53% of high-risk patients in the IFM 2018-04 trial achieved MRD negativity.
-
60% of high-risk patients in the GMMG-CONCEPT trial reached MRD negativity.
Achieving MRD negativity may be critical for a more durable response in high-risk myeloma patients.
Improving Outcomes for People with High-Risk Myeloma
Dr. Gay presented findings from two major trials, GMMG-HD7 and ISKiA, that tested the addition of isatuximab (Sarclisa) to standard induction treatments (VRd and KRd). The new quadruplet combinations, IsaVRD and IsaKRD, showed stronger responses compared to the triplet regimens for high-risk multiple myeloma patients.
In comparing high-risk patient outcomes based on the proteasome inhibitor used, no significant differences were found between carfilzomib (Kyprolis) and bortezomib (Velcade).
For high-risk myeloma patients, achieving a deep response is only part of the goal—it’s also critical to maintain that response over time. This makes the period after induction therapy especially important.
One of the biggest challenges remains for high-risk patients (and those with functional high-risk) who relapse shortly after what seems to be a strong response. Research in this area continues to be focused on identifying these patients earlier and adjusting treatment strategies to prevent these early relapses.
Quadruplet Induction Continues to Be the Standard of Care for Newly Diagnosed Patients
In summary, quadruplet therapy—including an anti-CD38 antibody, a proteasome inhibitor, an immunomodulatory drug, and dexamethasone—has proven to be both safe and highly effective for most newly diagnosed myeloma patients. This powerful approach is helping many achieve deep responses, bringing new hope to patients and their families.
Looking ahead, researchers are focusing on key goals:
-
Boosting response rates for those with higher-risk disease, so all patients have a better chance at achieving remission.
-
Maintaining long-term responses to help ensure a lasting remission and improved quality of life.
Identifying patients early who may need a tailored approach to treatment, setting them up for the best possible outcomes from the start.
As research advances, these goals bring us closer to ensuring every person diagnosed with multiple myeloma receives the most effective care for their unique needs.
Dr. Francecsa Gay presented important data surrounding multiple myeloma induction therapy at the International Myeloma Society (IMS) meeting in Rio de Janeiro, Brazil.
Read on to learn more about the goals of induction therapy, as well as open questions such as optimal treatment cycles and schedules and how to improve induction therapy outcomes for high-risk multiple myeloma.
Goals of Induction Therapy in Multiple Myeloma
The main goals of induction therapy in newly diagnosed multiple myeloma are to control the disease quickly and effectively while keeping side effects manageable. This first phase of treatment is essential to set up the best possible outcomes for what comes next, like a potential stem cell transplant.
The key goals of induction therapy include:
-
Quickly lowering the number of myeloma cells to gain fast control over the disease.
-
Achieving a deep response—ideally, a Very Good Partial Response (VGPR) or better, aiming for MRD negativity (no detectable myeloma cells).
-
Making sure treatment is well-tolerated, with minimal side effects.
-
Preparing for a successful stem cell harvest for patients who may be eligible for a stem cell transplant.
Achieving Deep Responses to Myeloma Therapy
Newly diagnosed myeloma patients can often achieve strong responses to induction therapy. The chart below highlights the average response levels patients can expect after completing their induction treatments.
Today’s myeloma treatment strategies make it possible for many patients to reach a VGPR (Very Good Partial Response) or even higher. Some induction therapies, especially quadruplet (4-drug) combinations, can lead to deep responses in a large portion of patients—often reaching minimal residual disease (MRD) negativity. This means that no myeloma cells are detected in a sample size as large as 100,000 to 1,000,000 cells, depending on the test.
Want to learn more about treatments and therapies for multiple myeloma from experts? Start watching HealthTree University videos here:
Safety in Induction Therapy
Fortunately, most induction therapies for newly diagnosed myeloma patients have a very low rate of discontinuation due to side effects, and treatment-related deaths during this phase are even rarer.
The primary concern for patients during this phase remains the risk of infections. This is due to both the immune system being compromised by myeloma itself and the side effects of treatment. Severe, life-threatening infections are uncommon at this stage.
Collecting Stem Cells: What to Expect
About 95-99% of multiple myeloma patients eligible for a stem cell transplant can successfully collect enough stem cells through a process called apheresis.
If anti-CD38 therapy (like daratumumab or isatuximab) is part of a patient’s four-drug induction therapy, they may collect slightly fewer stem cells than those on a three-drug regimen. However, 95% of patients still gather an adequate amount, so this isn’t typically a major concern.
Are you preparing for a stem cell transplant or curious about the process? Check out our stem cell transplant education guide here:
What’s Next for Myeloma Induction Therapy?
While the data presented above is promising, questions still remain such as:
-
What is the optimal number of treatment cycles for certain combinations? What’s the most efficient treatment schedule to get the best results?
and
-
What more can be done for high-risk myeloma patients whose responses tend to be shorter than those with standard-risk myeloma?
Optimizing Treatment Cycles and Schedules
Myeloma researchers have explored a six-cycle regimen with triplet (3-drug) therapies during induction, which has shown improvements in both response rates and depth, especially in helping patients reach VGPR (Very Good Partial Response). The next goal is to further boost these response rates by using quadruplet (4-drug) induction therapies.
In the recent GMMG-HD7 trial (shown on the right of the image above), a 12-week induction therapy achieved a 50% MRD negativity rate. This is the highest rate of such a deep response seen so far compared to other bortezomib (Velcade)--based quadruplet induction therapies.
The image above shows MRD-negative rates achieved with carfilzomib (Kyprolis)- based quadruplet induction therapies. Two trials, IFM 2018-04 and GMMG-CONCEPT, focused specifically on high-risk multiple myeloma patients and used an extended induction therapy of six 28-day cycles.
After this extended induction therapy:
-
53% of high-risk patients in the IFM 2018-04 trial achieved MRD negativity.
-
60% of high-risk patients in the GMMG-CONCEPT trial reached MRD negativity.
Achieving MRD negativity may be critical for a more durable response in high-risk myeloma patients.
Improving Outcomes for People with High-Risk Myeloma
Dr. Gay presented findings from two major trials, GMMG-HD7 and ISKiA, that tested the addition of isatuximab (Sarclisa) to standard induction treatments (VRd and KRd). The new quadruplet combinations, IsaVRD and IsaKRD, showed stronger responses compared to the triplet regimens for high-risk multiple myeloma patients.
In comparing high-risk patient outcomes based on the proteasome inhibitor used, no significant differences were found between carfilzomib (Kyprolis) and bortezomib (Velcade).
For high-risk myeloma patients, achieving a deep response is only part of the goal—it’s also critical to maintain that response over time. This makes the period after induction therapy especially important.
One of the biggest challenges remains for high-risk patients (and those with functional high-risk) who relapse shortly after what seems to be a strong response. Research in this area continues to be focused on identifying these patients earlier and adjusting treatment strategies to prevent these early relapses.
Quadruplet Induction Continues to Be the Standard of Care for Newly Diagnosed Patients
In summary, quadruplet therapy—including an anti-CD38 antibody, a proteasome inhibitor, an immunomodulatory drug, and dexamethasone—has proven to be both safe and highly effective for most newly diagnosed myeloma patients. This powerful approach is helping many achieve deep responses, bringing new hope to patients and their families.
Looking ahead, researchers are focusing on key goals:
-
Boosting response rates for those with higher-risk disease, so all patients have a better chance at achieving remission.
-
Maintaining long-term responses to help ensure a lasting remission and improved quality of life.
-
Identifying patients early who may need a tailored approach to treatment, setting them up for the best possible outcomes from the start.
As research advances, these goals bring us closer to ensuring every person diagnosed with multiple myeloma receives the most effective care for their unique needs.

about the author
Audrey Burton-Bethke
Audrey is a content writer and editor for the HealthTree Foundation. She originally joined the HealthTree Foundation in 2020. Audrey loves spending time with her supportive husband, energetic four-year-old, and new baby.
More on Treatment Advances






Trending Articles





Upcoming Events



Get the Latest Multiple Myeloma Updates, Delivered to You.
By subscribing to the HealthTree newsletter, you'll receive the latest research, treatment updates, and expert insights to help you navigate your health.
Together we care.
Together we cure.