ASH 2020: Real World Use of Minimal Residual Disease (MRD) Testing in Multiple Myeloma

How important is MRD testing for myeloma patients and what are the practical implications of using it in clinical trials as an earlier end-point? This is the question addressed at a Wednesday ASH 2020 workshop by several multiple myeloma specialists. Experts believe it is a useful and evolving tool.
Pierre Demolis, MD, PhD of the French Medicines Agency, EMA noted that the most important questions surrounding MRD are still:
- When should we measure MRD?
- Does depth of response matter?
- Does duration of response matter?
- Could MRD results predict response to treatment?
- Is the MRD result relevance the same if you test for an early stage vs. late stage patient?
- Would a semi-qualitative prediction work?
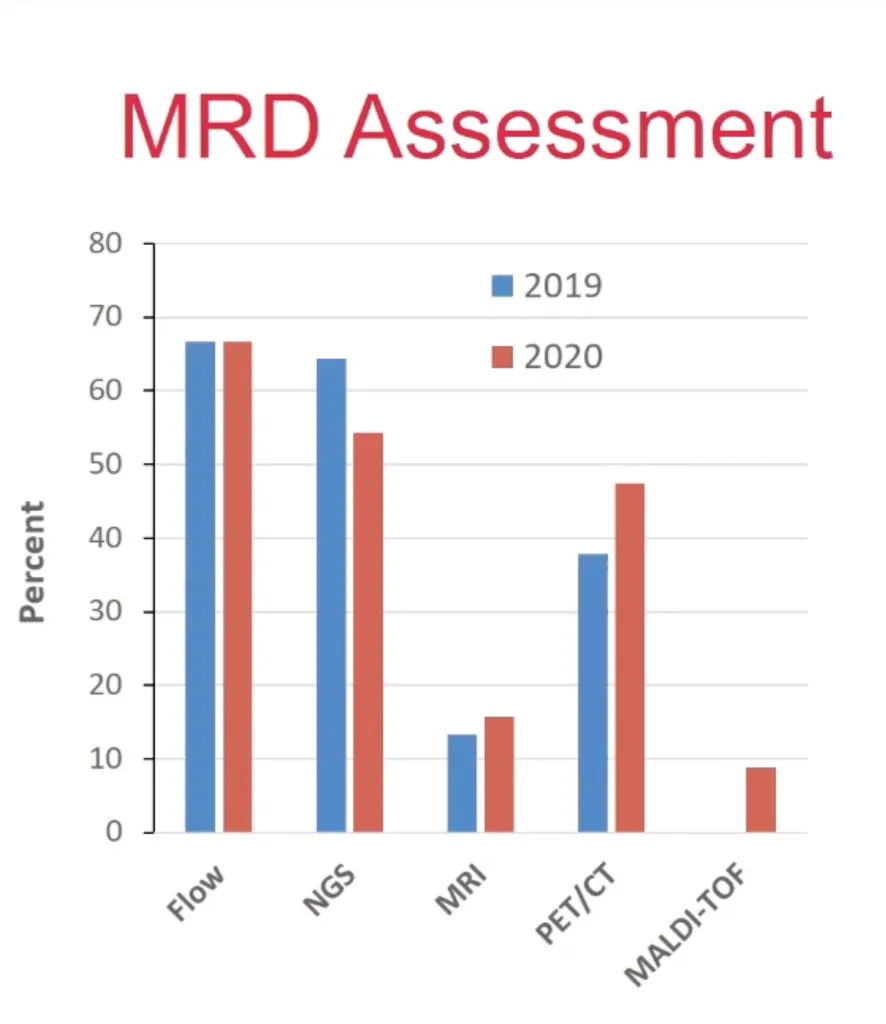
Sarah Holstein, MD of the University of Nebraska reviewed an MRD study of real world use of testing in myeloma. As you can see in the chart, the most common forms of MRD testing are flow cytometry and Next Generation Sequencing (NGS) testing. Using imaging to detect residual disease is also being used. In a Thursday ASH panel, myeloma experts stated that their preferred test was the NGS MRD test.
When asked if the use of MRD testing changed the way experts treated myeloma patients, 56% of specialists reported that it triggered a change in watching the movement of a patient's disease, but only 21% reported that it changed the way they treated the patient. Dr. Holstein noted that there has been an increase of MRD testing, but the tests still vary in type of test, sensitivity, timing and frequency. Only a minority of doctors are using it to guide treatment decisions.
Francesca Gay, MD, PhD of GIMEMA of the European Myeloma Network in Italy dove into the details of a real-world clinical trial that used MRD testing to see which arm of a trial was better:
- Kyprolis/Rev/Dex + stem cell transplant (KRD + SCT)
- Kyprolis/Cyclophosphamide/Dex + stem cell transplant (KCD + SCT)
- Kyprolis/Rev/Dex for 12 months and no transplant (KRD)
The KRD plus transplant arm was the winner with a higher rate of sustained MRD negativity and better progression free survival.
| KRD+ SCT | KRD | KCD + SCT | |
| Rate of sustained MRD | 68% | 54% | 45% |
| Progression free survival | 78% | 66% | 58% |
Patients in the FORTE trial were split between two different maintenance arms - one using Kyprolis/Revlimid and the other using Revlimid alone. Patients who moved from MRD positive to MRD negative during maintenance was higher in the KR arm (46%) compared to the Revlimid arm (32%) and the KR maintenance arm also improved progression free survival (81%) compared to the Revlmid alone (68%). This suggests that using the KR combination as maintenance is much more likely to provide longer lasting remissions but expert in the Thursday panel noted that it also could increase toxicity.
The chart below shows that even for MRD negative patients, the KR arm was still better than Revlimid alone. Dr. Gay also noted that the MRD results were similar for high risk patients as well as standard risk patients.

In conclusion, the myeloma community agrees that MRD testing will continue to be included in clinical trials. This additional data will help us understand the answers to the lingering questions.
Related ASH 2020 Articles
- ASH 2020: Real world use of MRD testing in multiple myeloma
- ASH 2020: Multiple myeloma and the gut microbiome
- ASH 2020: Top 7 myeloma abstracts according to myeloma specialists
- ASH 2020: Dr. Vincent Rajkumar's top myeloma abstracts
- ASH 2020: Fauci opens ASH with Reflections on COVID-19
- ASH 2020: Managing CAR T Side Effects in Multiple Myeloma
How important is MRD testing for myeloma patients and what are the practical implications of using it in clinical trials as an earlier end-point? This is the question addressed at a Wednesday ASH 2020 workshop by several multiple myeloma specialists. Experts believe it is a useful and evolving tool.
Pierre Demolis, MD, PhD of the French Medicines Agency, EMA noted that the most important questions surrounding MRD are still:
- When should we measure MRD?
- Does depth of response matter?
- Does duration of response matter?
- Could MRD results predict response to treatment?
- Is the MRD result relevance the same if you test for an early stage vs. late stage patient?
- Would a semi-qualitative prediction work?
Sarah Holstein, MD of the University of Nebraska reviewed an MRD study of real world use of testing in myeloma. As you can see in the chart, the most common forms of MRD testing are flow cytometry and Next Generation Sequencing (NGS) testing. Using imaging to detect residual disease is also being used. In a Thursday ASH panel, myeloma experts stated that their preferred test was the NGS MRD test.
When asked if the use of MRD testing changed the way experts treated myeloma patients, 56% of specialists reported that it triggered a change in watching the movement of a patient's disease, but only 21% reported that it changed the way they treated the patient. Dr. Holstein noted that there has been an increase of MRD testing, but the tests still vary in type of test, sensitivity, timing and frequency. Only a minority of doctors are using it to guide treatment decisions.
Francesca Gay, MD, PhD of GIMEMA of the European Myeloma Network in Italy dove into the details of a real-world clinical trial that used MRD testing to see which arm of a trial was better:
- Kyprolis/Rev/Dex + stem cell transplant (KRD + SCT)
- Kyprolis/Cyclophosphamide/Dex + stem cell transplant (KCD + SCT)
- Kyprolis/Rev/Dex for 12 months and no transplant (KRD)
The KRD plus transplant arm was the winner with a higher rate of sustained MRD negativity and better progression free survival.
| KRD+ SCT | KRD | KCD + SCT | |
| Rate of sustained MRD | 68% | 54% | 45% |
| Progression free survival | 78% | 66% | 58% |
Patients in the FORTE trial were split between two different maintenance arms - one using Kyprolis/Revlimid and the other using Revlimid alone. Patients who moved from MRD positive to MRD negative during maintenance was higher in the KR arm (46%) compared to the Revlimid arm (32%) and the KR maintenance arm also improved progression free survival (81%) compared to the Revlmid alone (68%). This suggests that using the KR combination as maintenance is much more likely to provide longer lasting remissions but expert in the Thursday panel noted that it also could increase toxicity.
The chart below shows that even for MRD negative patients, the KR arm was still better than Revlimid alone. Dr. Gay also noted that the MRD results were similar for high risk patients as well as standard risk patients.
In conclusion, the myeloma community agrees that MRD testing will continue to be included in clinical trials. This additional data will help us understand the answers to the lingering questions.
Related ASH 2020 Articles
- ASH 2020: Real world use of MRD testing in multiple myeloma
- ASH 2020: Multiple myeloma and the gut microbiome
- ASH 2020: Top 7 myeloma abstracts according to myeloma specialists
- ASH 2020: Dr. Vincent Rajkumar's top myeloma abstracts
- ASH 2020: Fauci opens ASH with Reflections on COVID-19
- ASH 2020: Managing CAR T Side Effects in Multiple Myeloma

about the author
Jennifer Ahlstrom
Myeloma survivor, patient advocate, wife, mom of 6. Believer that patients can contribute to cures by joining HealthTree Cure Hub and joining clinical research. Founder and CEO of HealthTree Foundation.
More on Conferences















Get the Latest Multiple Myeloma Updates, Delivered to You.
By subscribing to the HealthTree newsletter, you'll receive the latest research, treatment updates, and expert insights to help you navigate your health.
Together we care.
Together we cure.