ASH 2023: Raising the BCMA Standard in Multiple Myeloma
A very exciting and informative educational series occurred at ASH 2023 on BCMA-targeting products by a panel of experts.
The program was sponsored by Janssen Biotech, Inc., administered by Janssen Scientific Affairs, LLC, Pfizer, and Regeneron Pharmaceuticals, Inc.
This CME/MOC/AAPA activity is provided by PeerView Institute for Medical Education and developed with our favorite educational partner HealthTree Foundation for Multiple Myeloma.
You can watch the replay of this powerful session here: Raising the BCMA Standard in Multiple Myeloma: Strategies for Enhanced Care With Potent CAR-T and Bispecific Options
You may have to take a short survey before viewing the replay.
Nikhil C. Munshi, MD, kicked off the discussion, sharing the exciting progress of immunotherapies in general, and focused heavily on CAR-T.
BCMA-Directed Immunotherapies and CAR-T Treatment
Just over a year ago, myeloma researchers were happy when clinical trial results had a 30 percent overall response rate in clinical trials.
With recent FDA approvals of CAR T-cell products and bispecific antibody therapy products, myeloma researchers are looking at response rates of 60 percent overall response rates or higher for just a single agent (meaning, that the medications were not combined).
These BCMA-targeting products are an important step forward in treating multiple myeloma.
- Belantamab mafodotin (BLENREP)
- Idecabtagene vicleucel (Ide-cel, a CAR T-cell product)
- Ciltacabtagene autoleucel (Cital-cel, a CAR T-cell product)
- Teclistamab (bispecific antibody therapy)
- Elranatamab (bispecific antibody therapy)
Dr. Munshi discussed in detail the studies leading to these approvals.
He then asked a pressing question to the panel of his specialists: Does the age of a myeloma patient matter when considering CAR T-cell therapy?
There was a resounding "no" from all of the specialists. However, they do consider comorbidities, functional status, and renal function.
Throughout the presentation, there was information about the management of CAR-T, with the end goal of preventing neurotoxicity and cytokine release syndrome (CRS), which can result in multisystem organ failure, but do not stop the CAR-T cells from working.
He also discussed treatment for CRS and supportive care with tocilizumab and steroids.
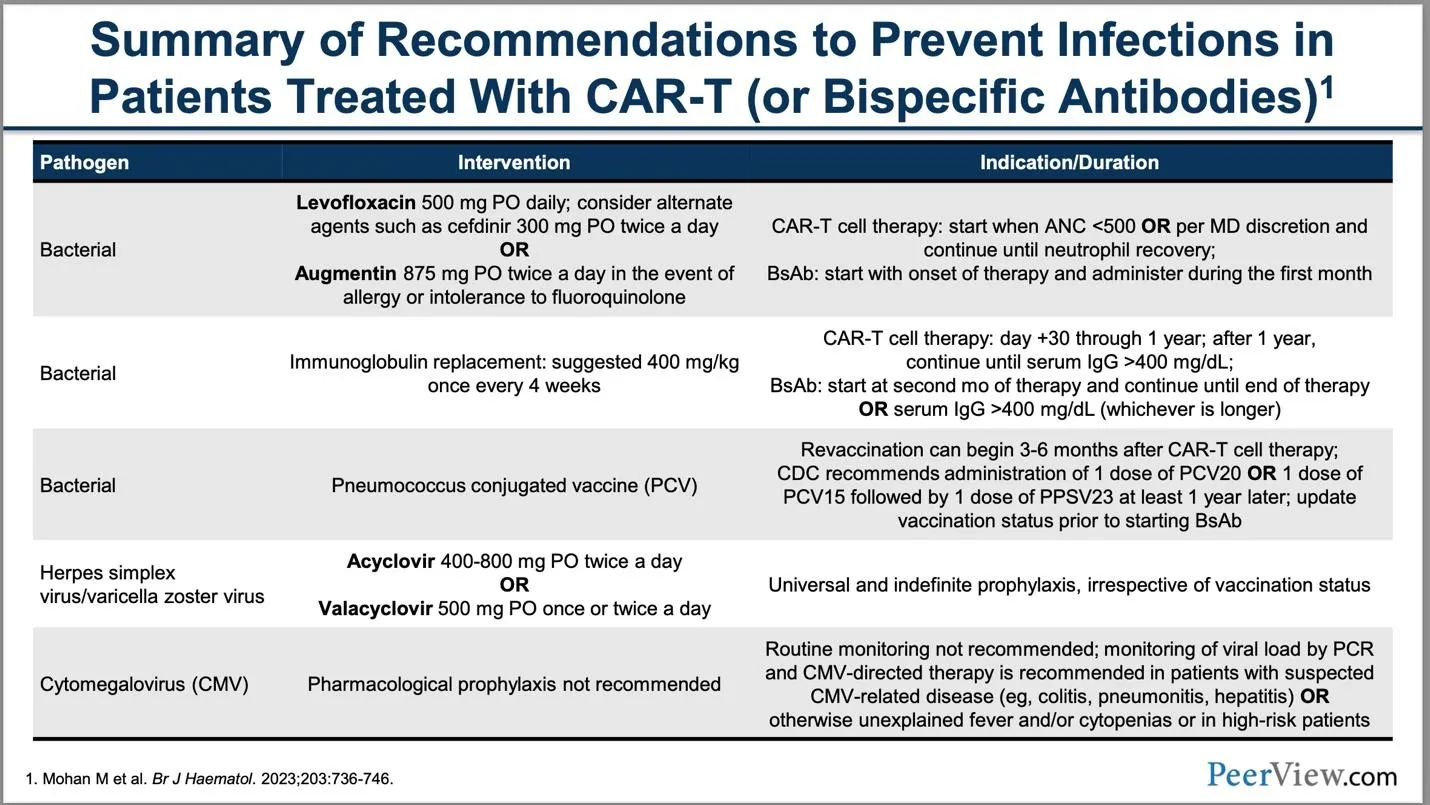
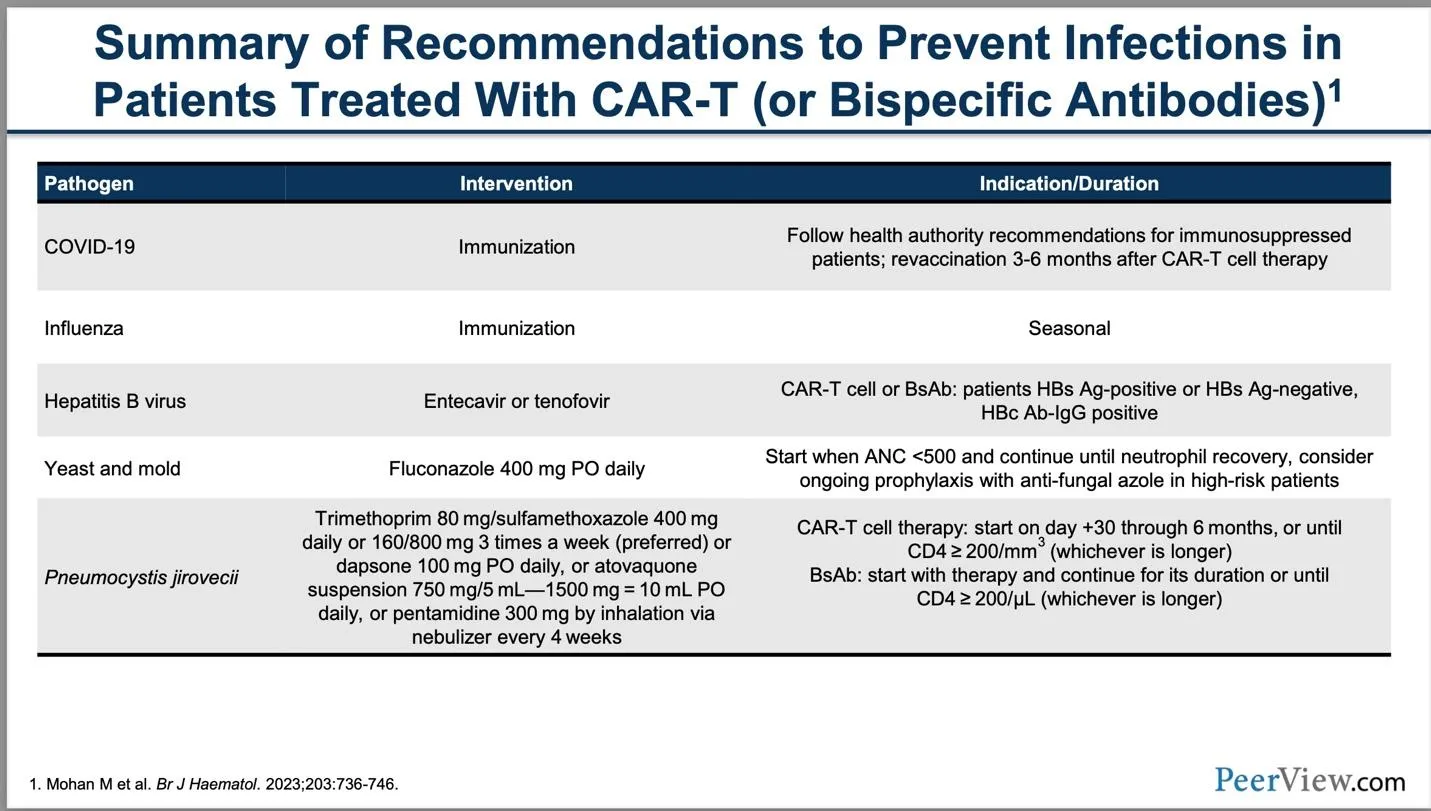
He gave this helpful summary of recommendations to prevent infection in CAR T-cell therapy that can also be used for bispecific antibody therapies.
Please see the detailed charts from the presentation below.
In closing Dr. Munshi talked about the future of immunotherapy treatments:
- Dual antigen binding (2 targets in 1 Car-T product)
- RNA CAR products
- T-cells stimulated with a vaccine
- Seeking new targets for immunotherapies
- Faster CAR-T production (currently takes 4-8 weeks)
- Earlier line treatment
- Possible re-treatment at progression
- Improved protocols for treatment
The Future of CAR-T Therapy
Dr. Krina Patel MD, MSc was the next speaker. She expressed her hope about the future of CAR-T. She discussed the CARTITUDE-4 study and how it may help move CAR-T earlier in treatment lines.
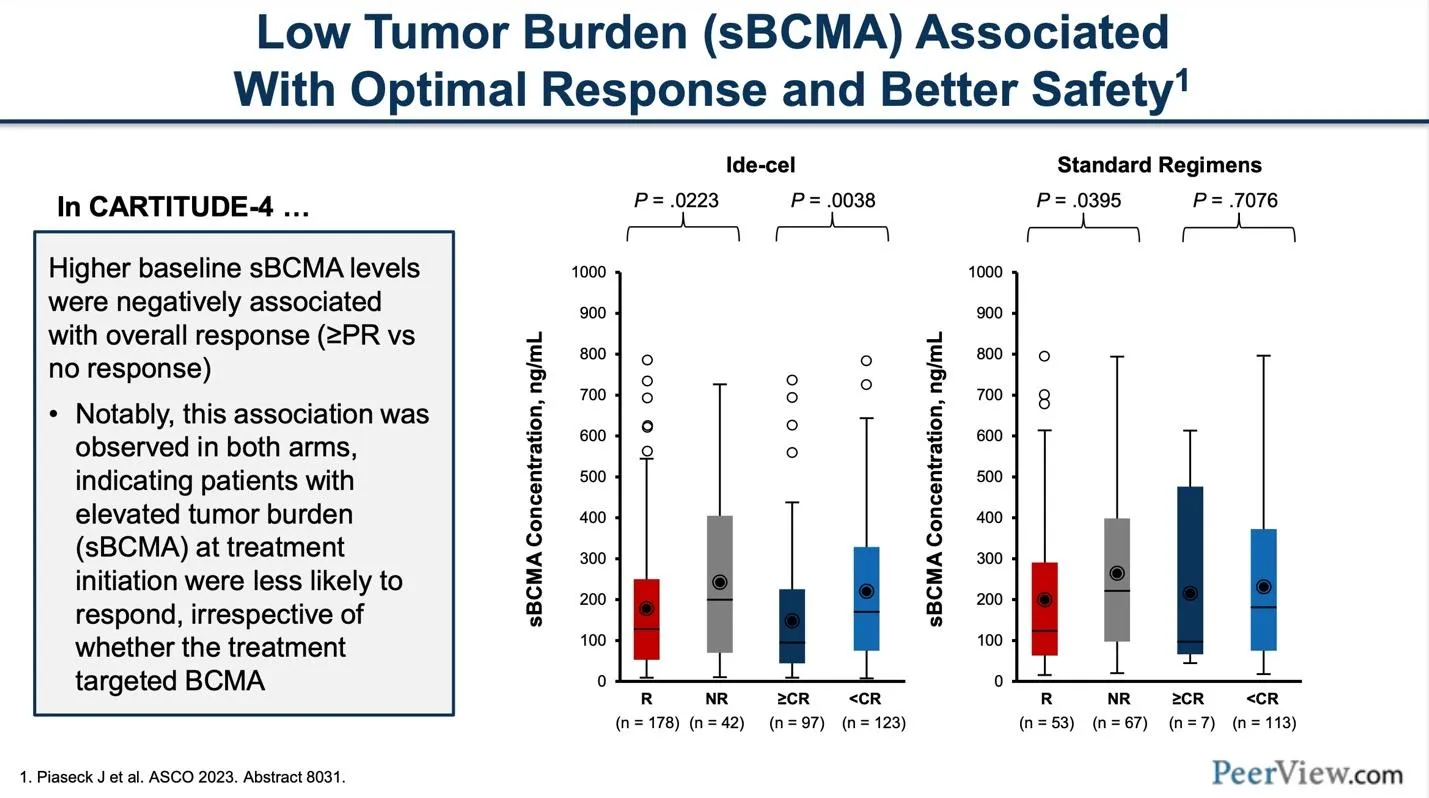
CAR-T therapy treatment, Dr. Patel shares, is effective for high-risk patients. Specifically, lower tumor burden makes for better outcomes and less cytokine release syndrome, so bridging therapy after apheresis is important.
The chart below details/ summarizes these differences:
The next items on Dr. Patel's agenda were the up-and-coming immune therapies:
- Novel FasT Car-T, which is a dual target Car-T. This is still in clinical trials, and the two targets are BCMA and CD19. Ideally with two targets, this could allow for a more potent and durable therapy, such as combination therapies.
- Durcabtagene autoleucel: a product manufactured using a platform that decreases production time to about 24 hours and takes less than two days to manufacture. This clinical trial product has the ability to expand after CAR-T cell infusion.
In summary, Dr. Patel hopes the current evidence supports the earlier use of CAR-T in treatment. This includes lenalidomide refractory and high-risk patients. Dr. Patel expressed the hope that everyone can get CAR-T therapy. The new products mentioned above would help push the field forward.
Bispecific Antibody Therapies
Dr. Mohamad Monty was the third speaker. His discussion was on the FDA-approved bispecific therapy antibodies. He began with a review of studies that led to FDA approval of the bispecifics known as teclistamab and elranatamab, both of which target BCMA.
Unlike CAR-T products that need more time to manufacture, these products are off the shelf and ready to go.
Both elranatamab and teclistimab have very good response rates at over 60%. However, these response rates do drop in patients with high disease burden and extramedullary disease.
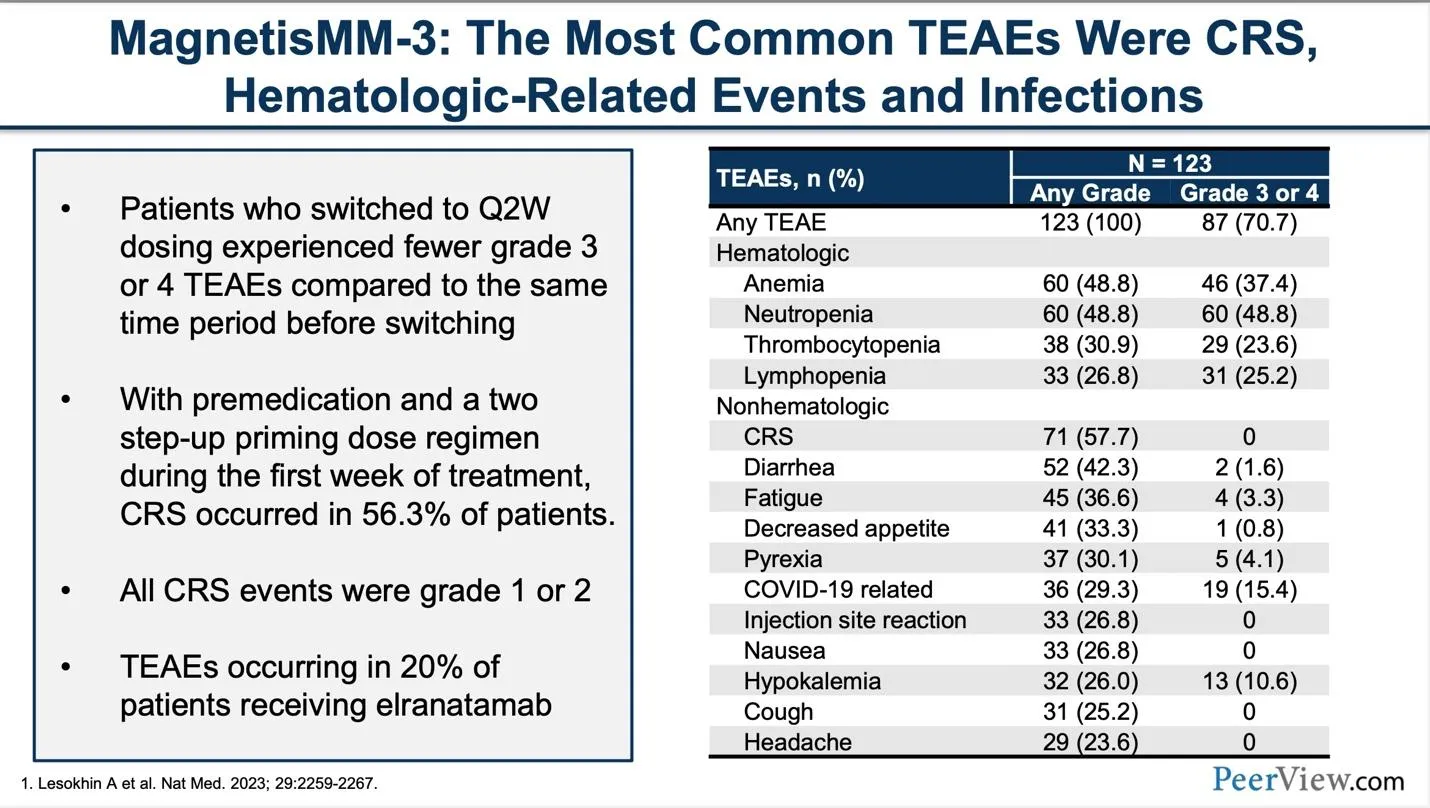
Dr. Monty reviewed the details about step-up dosing and dosing schedules for the bispecific antibody therapies. Then, he detailed the side effects: cytopenia or low blood counts, infections, and cytokine release syndrome (CRS). He reports CRS usually occurs within the first 3 doses. These side effects are listed in the chart below from the MagnetisMM-3 study.
He discussed the relatively new FDA-approved GPRC5D targeted bispecific antibody, talquetamab. While it doesn't target BCMA, it's a great therapy to use after a patient relapses after a BCMA-targeting CAR-T or bispecific antibody.
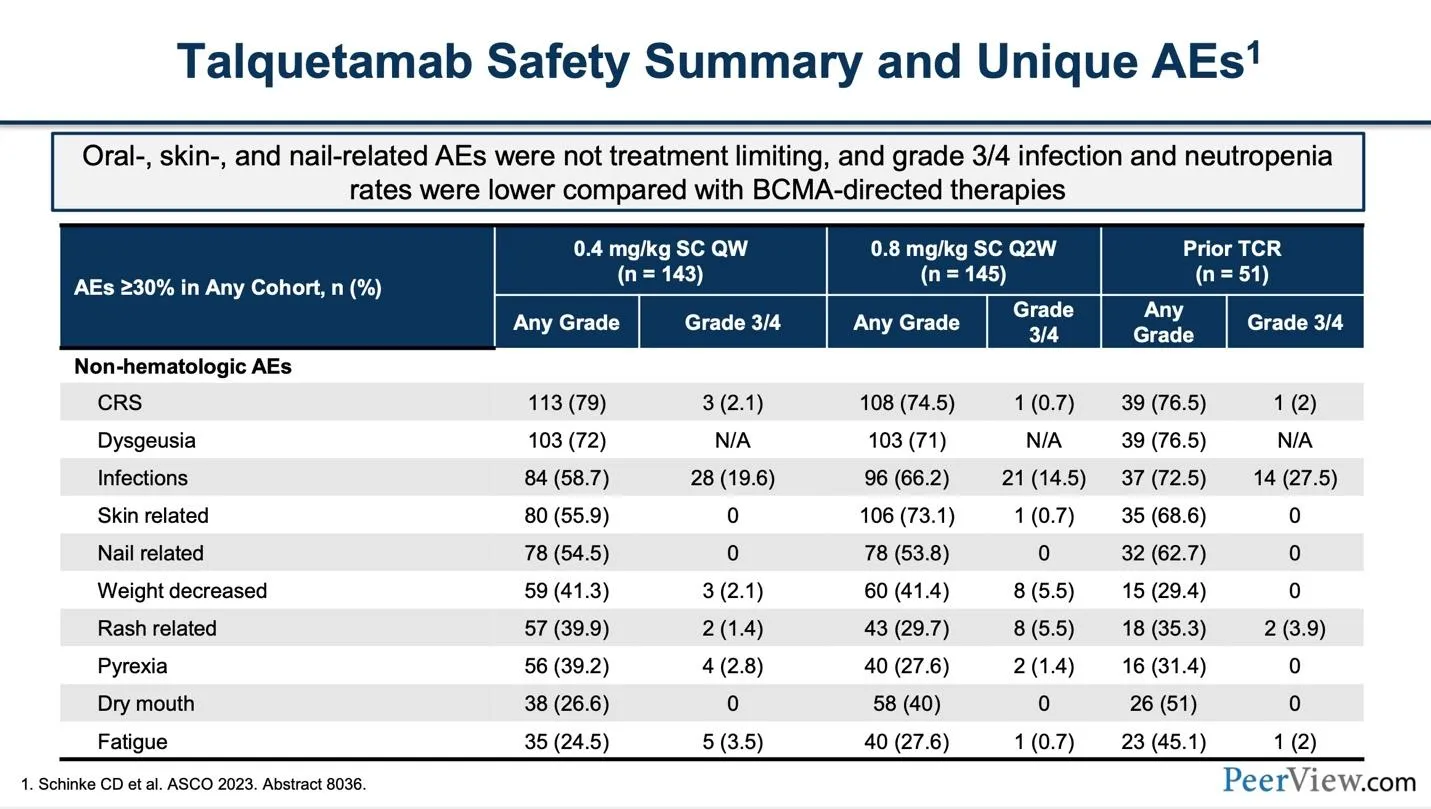
The overall response rate for talquetamab was 73% but lower with a past bispecific antibody. It has side effects like dysgeusia which is altered taste and skin/nail issues as seen in this table:
The preliminary data of combining teclistamab (BCMA) and talquetamab (GPRC5D) bispecific products was particularly interesting. This combination produced an overall response rate of 96% (way above the previous standard of 30%) and an 86% overall response rate in the extramedullary disease subgroups. The safety profile remained the same with no further complications.
In summary, bispecifics can be readily available to qualifying patients and can be very effective for the right candidate. Preventative infection management by your myeloma specialist is important as these products have unique toxicities that must be monitored.
The Future of Bispecific Antibodies
Hans Lee, MD, presented blazing a new trail in relapsed multiple myeloma with these new products that are now in clinical trials:
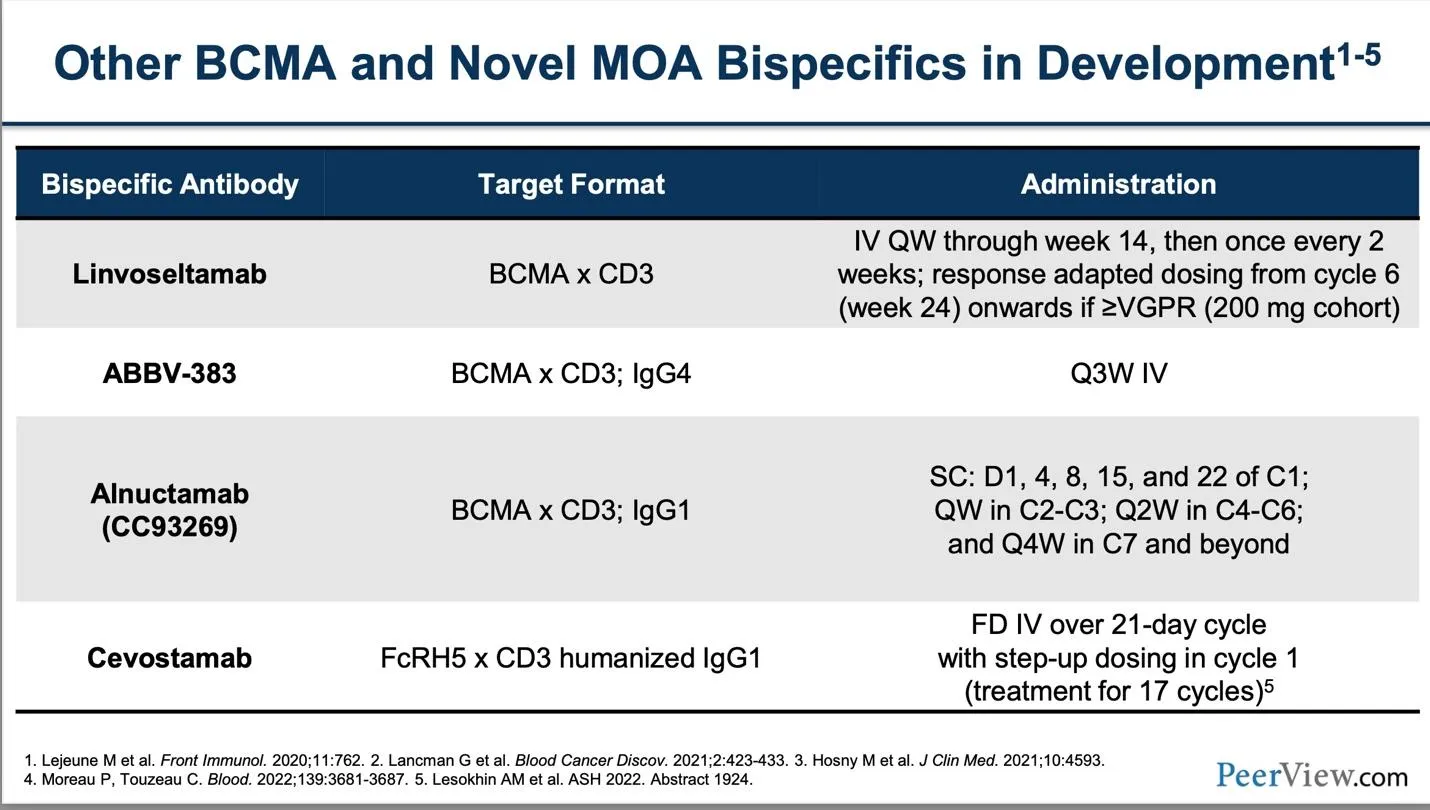
Linvoseltamab is another BCMA-directed bispecific antibody therapy with an overall response rate of 71%. The progression-free survival (PFS) has not been reached yet for this specific clinical trial.
Alnuctamab is a bivalent binding bispecific antibody. This means that it attaches in two places to the BCMA antigen. They are testing different dosages and have a total of 73 patients with an overall response rate (ORR) ranging from 54% to 69% with a follow-up time of 7.4 months.
ABBV-383 is a fully humanized product. They are still trying to determine the best dosing and have tested three dosage levels with a response rate ranging from 44% to 60%. Progression-free survival and duration of response have not yet been reached.
Cevostamab has a different target protein called FcRH5 and shows response rates after BCMA therapy of 56.7% at the 132-198 mg higher dose level compared to 36.1 % at the 20-90 mg dose level. This is a groundbreaking immunotherapy with durable results.
In summary, there are several promising products in development that are still in the clinical trials phase. They have different modes of administration, dosing schedules, and side effect profiles.
These researchers are working hard to understand these new products and maximize these treatments to deliver the best results for multiple myeloma patients. The Healthtree Coaches would like to thank them for their work/sharing their progress.
Subscribe to the HealthTree Newsletter for more future informationon these new products.
ASH 2023 Resources
Would you like to watch ASH 2023 myeloma research interviews from the investigators themselves? Click "ASH 2023" here: HealthTree University Conference Coverage
To read other ASH 2023 articles, click here: HealthTree 2023 ASH Articles
A very exciting and informative educational series occurred at ASH 2023 on BCMA-targeting products by a panel of experts.
The program was sponsored by Janssen Biotech, Inc., administered by Janssen Scientific Affairs, LLC, Pfizer, and Regeneron Pharmaceuticals, Inc.
This CME/MOC/AAPA activity is provided by PeerView Institute for Medical Education and developed with our favorite educational partner HealthTree Foundation for Multiple Myeloma.
You can watch the replay of this powerful session here: Raising the BCMA Standard in Multiple Myeloma: Strategies for Enhanced Care With Potent CAR-T and Bispecific Options
You may have to take a short survey before viewing the replay.
Nikhil C. Munshi, MD, kicked off the discussion, sharing the exciting progress of immunotherapies in general, and focused heavily on CAR-T.
BCMA-Directed Immunotherapies and CAR-T Treatment
Just over a year ago, myeloma researchers were happy when clinical trial results had a 30 percent overall response rate in clinical trials.
With recent FDA approvals of CAR T-cell products and bispecific antibody therapy products, myeloma researchers are looking at response rates of 60 percent overall response rates or higher for just a single agent (meaning, that the medications were not combined).
These BCMA-targeting products are an important step forward in treating multiple myeloma.
- Belantamab mafodotin (BLENREP)
- Idecabtagene vicleucel (Ide-cel, a CAR T-cell product)
- Ciltacabtagene autoleucel (Cital-cel, a CAR T-cell product)
- Teclistamab (bispecific antibody therapy)
- Elranatamab (bispecific antibody therapy)
Dr. Munshi discussed in detail the studies leading to these approvals.
He then asked a pressing question to the panel of his specialists: Does the age of a myeloma patient matter when considering CAR T-cell therapy?
There was a resounding "no" from all of the specialists. However, they do consider comorbidities, functional status, and renal function.
Throughout the presentation, there was information about the management of CAR-T, with the end goal of preventing neurotoxicity and cytokine release syndrome (CRS), which can result in multisystem organ failure, but do not stop the CAR-T cells from working.
He also discussed treatment for CRS and supportive care with tocilizumab and steroids.
He gave this helpful summary of recommendations to prevent infection in CAR T-cell therapy that can also be used for bispecific antibody therapies.
Please see the detailed charts from the presentation below.
In closing Dr. Munshi talked about the future of immunotherapy treatments:
- Dual antigen binding (2 targets in 1 Car-T product)
- RNA CAR products
- T-cells stimulated with a vaccine
- Seeking new targets for immunotherapies
- Faster CAR-T production (currently takes 4-8 weeks)
- Earlier line treatment
- Possible re-treatment at progression
- Improved protocols for treatment
The Future of CAR-T Therapy
Dr. Krina Patel MD, MSc was the next speaker. She expressed her hope about the future of CAR-T. She discussed the CARTITUDE-4 study and how it may help move CAR-T earlier in treatment lines.
CAR-T therapy treatment, Dr. Patel shares, is effective for high-risk patients. Specifically, lower tumor burden makes for better outcomes and less cytokine release syndrome, so bridging therapy after apheresis is important.
The chart below details/ summarizes these differences:
The next items on Dr. Patel's agenda were the up-and-coming immune therapies:
- Novel FasT Car-T, which is a dual target Car-T. This is still in clinical trials, and the two targets are BCMA and CD19. Ideally with two targets, this could allow for a more potent and durable therapy, such as combination therapies.
- Durcabtagene autoleucel: a product manufactured using a platform that decreases production time to about 24 hours and takes less than two days to manufacture. This clinical trial product has the ability to expand after CAR-T cell infusion.
In summary, Dr. Patel hopes the current evidence supports the earlier use of CAR-T in treatment. This includes lenalidomide refractory and high-risk patients. Dr. Patel expressed the hope that everyone can get CAR-T therapy. The new products mentioned above would help push the field forward.
Bispecific Antibody Therapies
Dr. Mohamad Monty was the third speaker. His discussion was on the FDA-approved bispecific therapy antibodies. He began with a review of studies that led to FDA approval of the bispecifics known as teclistamab and elranatamab, both of which target BCMA.
Unlike CAR-T products that need more time to manufacture, these products are off the shelf and ready to go.
Both elranatamab and teclistimab have very good response rates at over 60%. However, these response rates do drop in patients with high disease burden and extramedullary disease.
Dr. Monty reviewed the details about step-up dosing and dosing schedules for the bispecific antibody therapies. Then, he detailed the side effects: cytopenia or low blood counts, infections, and cytokine release syndrome (CRS). He reports CRS usually occurs within the first 3 doses. These side effects are listed in the chart below from the MagnetisMM-3 study.
He discussed the relatively new FDA-approved GPRC5D targeted bispecific antibody, talquetamab. While it doesn't target BCMA, it's a great therapy to use after a patient relapses after a BCMA-targeting CAR-T or bispecific antibody.
The overall response rate for talquetamab was 73% but lower with a past bispecific antibody. It has side effects like dysgeusia which is altered taste and skin/nail issues as seen in this table:
The preliminary data of combining teclistamab (BCMA) and talquetamab (GPRC5D) bispecific products was particularly interesting. This combination produced an overall response rate of 96% (way above the previous standard of 30%) and an 86% overall response rate in the extramedullary disease subgroups. The safety profile remained the same with no further complications.
In summary, bispecifics can be readily available to qualifying patients and can be very effective for the right candidate. Preventative infection management by your myeloma specialist is important as these products have unique toxicities that must be monitored.
The Future of Bispecific Antibodies
Hans Lee, MD, presented blazing a new trail in relapsed multiple myeloma with these new products that are now in clinical trials:
Linvoseltamab is another BCMA-directed bispecific antibody therapy with an overall response rate of 71%. The progression-free survival (PFS) has not been reached yet for this specific clinical trial.
Alnuctamab is a bivalent binding bispecific antibody. This means that it attaches in two places to the BCMA antigen. They are testing different dosages and have a total of 73 patients with an overall response rate (ORR) ranging from 54% to 69% with a follow-up time of 7.4 months.
ABBV-383 is a fully humanized product. They are still trying to determine the best dosing and have tested three dosage levels with a response rate ranging from 44% to 60%. Progression-free survival and duration of response have not yet been reached.
Cevostamab has a different target protein called FcRH5 and shows response rates after BCMA therapy of 56.7% at the 132-198 mg higher dose level compared to 36.1 % at the 20-90 mg dose level. This is a groundbreaking immunotherapy with durable results.
In summary, there are several promising products in development that are still in the clinical trials phase. They have different modes of administration, dosing schedules, and side effect profiles.
These researchers are working hard to understand these new products and maximize these treatments to deliver the best results for multiple myeloma patients. The Healthtree Coaches would like to thank them for their work/sharing their progress.
Subscribe to the HealthTree Newsletter for more future informationon these new products.
ASH 2023 Resources
Would you like to watch ASH 2023 myeloma research interviews from the investigators themselves? Click "ASH 2023" here: HealthTree University Conference Coverage
To read other ASH 2023 articles, click here: HealthTree 2023 ASH Articles

about the author
Beth Travis
Beth is a licensed Physical Therapist that truly believes in the benefits of exercise. Mother of two, a myeloma patient and advocate with a love of learning, healthy lifestyles and food adventures.





Trending Articles



Upcoming Events



Get the Latest Multiple Myeloma Updates, Delivered to You.
By subscribing to the HealthTree newsletter, you'll receive the latest research, treatment updates, and expert insights to help you navigate your health.
Together we care.
Together we cure.