ASH 2023: How Can Relapsed/Refractory Myeloma Outcomes Improve in 2024?

I had a front-row seat for an educational seminar at ASH in which three specialists took a new look at current evidence that reflects best practices for relapsed and refractory multiple myeloma patient treatments.
Throughout the program, the presenters focused on three areas in which relapsed and refractory outcomes for multiple myeloma patients can improved:
- A rational approach to functional high-risk patients
- Considerations for the next therapy after anti-CD38 monoclonal antibodies used as first-line
- Options at the time of relapse after anti-BCMA therapy
Dr. Francesa Gay, MD, PhD began the session by discussing functional high-risk multiple myeloma.
Functional High-Risk Myeloma Patients
Functional high-risk patients can be defined as those who are not identified as high-risk at original diagnosis, but after standard-of-care treatments, relapse faster than the average myeloma patient, often within 12-18 months of their optimal initial therapy.
These patients can be treated with standard treatments such as immunomodulatory agents, proteasome inhibitors, and monoclonal antibodies. Other treatment options include novel therapies such as CAR-T cells, bispecific antibodies, and antibody-drug conjugates.
The table below shows articles or papers that dive into this issue. All of these tests were done on patients using, newer, standard-of-care treatments. However, the rate of earlier relapse ranges from 10-40%.
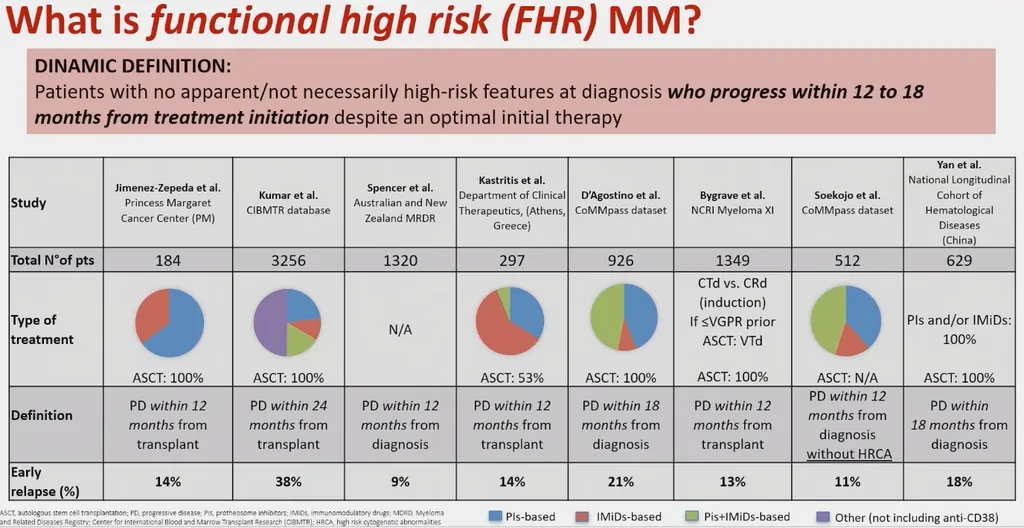
Despite the different reports and different treatments, the median overall survival for functional high-risk patients is two years. This is significantly inferior to the overall survival of those with standard myeloma that are often living over a decade.
There is a high medical need to find successful treatments or treatment sequencing for these patients as their post-relapse survival rates have not improved since 2005, despite the novel therapies that are being developed and approved at a rapid pace.
The problem is identifying the functional high-risk myeloma patients before they relapse, something quite difficult to do considering most patients aren’t classified as functional high-risk until they are relapsing early, and 10-20% of the myeloma patients who are functionally high risk have no classic high-risk indications (such as high tumor burden, high-risk mutations, or advanced ISS staging).
One predictor for identifying functionally high-risk patients lies in the quality of response that they have to their standard-of-care treatments. Those with suboptimal responses, for example not achieving VGPR or CR after their induction therapy, are more likely to be classified as high-risk.
It’s also important to note that patients can change their risk status. In fact, in one highlighted study 54% of patients changed their risk status after 9 months.
How can functionally high-risk patients be managed when they relapse “early”?
The majority of these patients are refractory to previous treatments. Refractory status can be defined as a disease that becomes nonresponsive or progressive on therapy within 60 days of the last treatment. Patients usually achieve minimal responses to these therapies.
This makes treating these patients more difficult as they have fewer options available to them that can effectively fight their myeloma. A myeloma specialist can help you navigate your care when considering the various options for myeloma treatment as detailed at this link: Myeloma Treatment Options (HealthTree)
It makes the most sense to treat functional high-risk myeloma patients after relapse with a change in drug class. An example of a possible treatment algorithm for functional high-risk patients can be seen below:
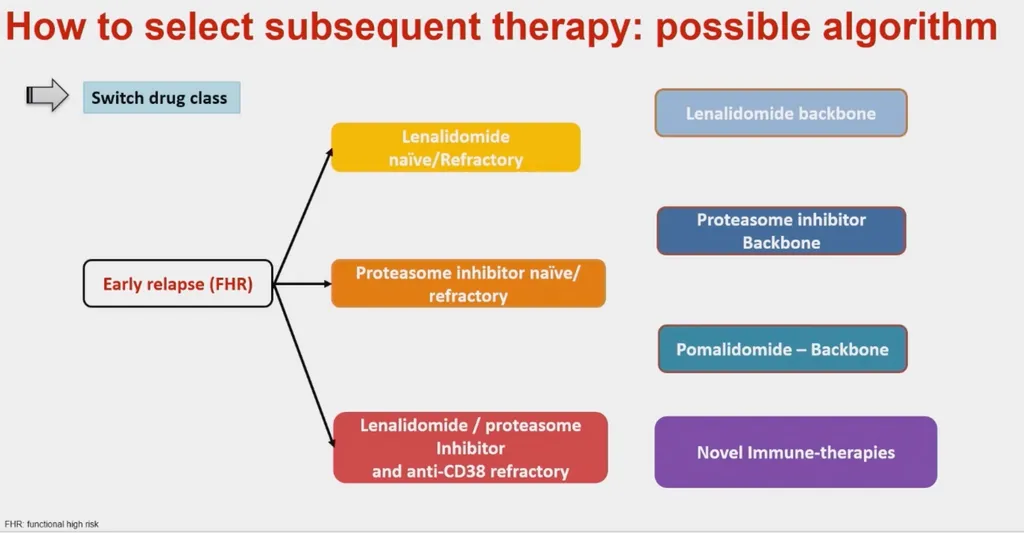
Dr. Gay presented several options for clinicians in charge of treating patients. There are options for first relapse options in lenalidomide naive patients: proteasome inhibitors backbone, or early immunotherapy.
This is a moment to stop and reinforce the lifesaving importance of having a myeloma specialist on your team. They are in tune with the newest research and can help you make key decisions in your treatment sequencing that can prolong your life and significantly improve the quality. Check out our specialist directory here: Multiple Myeloma Specialist Directory
Considerations for Next Therapy After Anti-CD38 Monoclonal Antibodies Used As First-Line
Dr. Monique Hartley-Brown's focus was improving treatment for relapsed/refractory multiple myeloma patients after anti-CD38 therapy exposure in their first line of therapy.
As a reminder, CD38 is highly expressed on multiple myeloma cells, and functions as a receptor (adhesion molecule) that mediates immunosuppression. CD38 is expressed in the bone marrow microenvironment and is also expressed by immune cells, such as T-cells, NK cells, and more.
CD38 is therefore a critical target in multiple myeloma therapy, and anti-CD38 monoclonal antibodies used to treat myeloma are truly transforming newly diagnosed myeloma treatment. For more information on monoclonal antibody treatments for multiple myeloma, check them out here: Monoclonal Antibody Myeloma Treatments (HealthTree)
There are two anti-CD38 monoclonal antibodies that are currently FDA-approved for myeloma treatment, isatuximab and daratumamab. They work slightly differently from each other, and could possibly be valuable as complementary/alternative therapies to one another.
After the published GRIFFIN study (as seen below), several multiple myeloma specialists and even specialist centers have started to change their standard-of-care induction therapies for newly diagnosed multiple myeloma patients to include anti-CD38 therapies.
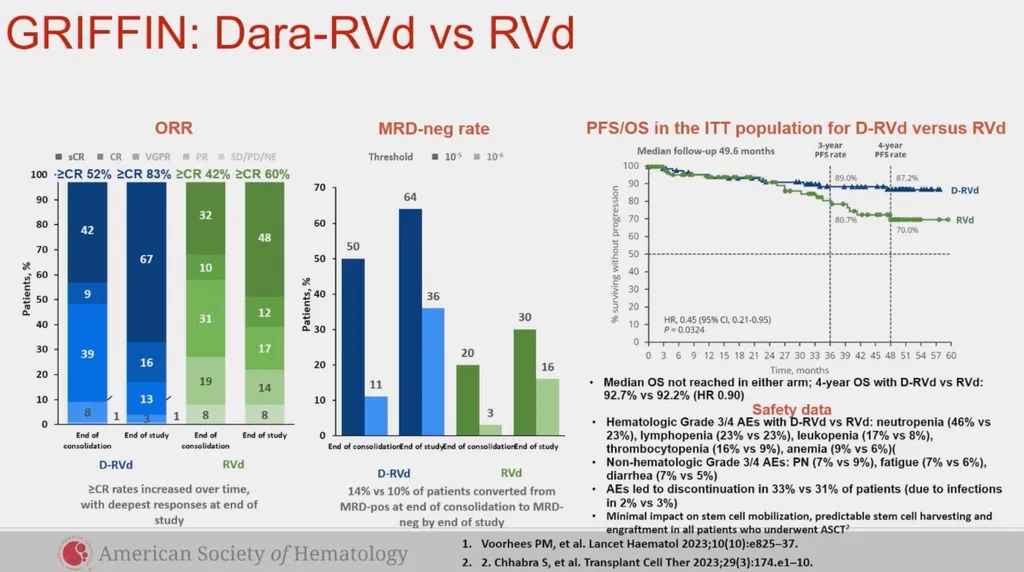
Even at this particular ASH conference, there was a lot of excitement and interest surrounding the findings of isatuximab and its ability to get many patients into MRD (minimal residual disease) negativity.
Other key clinical trials such as the MAIA trial and the Phase III trial PERSEUS (which was also presented with much anticipation at this ASH conference) have proven the effectiveness of adding an anti-CD38 monoclonal antibody as shown in the GRIFFIN study.
Many more clinical trials testing various versions of an induction quadrupled with an anti-CD38 monoclonal antibody are currently in the pipeline.
Because more patients are receiving anti-CD38 myeloma therapies upfront, the question remains of how/with which therapies to treat these patients when the disease begins to progress. What are viable and effective second and third line therapies for patients that are in this situation?
- A deferred stem cell transplant could be a great option for these patients. An upfront transplant doesn't offer any overall survival benefits, so "saving" the stem cell transplant for a further line of therapy instead of including it as a part of the induction/consolidation therapy might be the right answer for a selection of patients.
- Another option could be the use of selinexor, bortezomib and dexamethasone could be an option for a patient in this situation. Findings in the BOSTON trial showed this combination to be more successful than combining bortezomib and dexamethasone alone.
- BCMA-targeted therapies such as CAR-T therapy or bispecific antibodies like teclistimab or elranatamab could be a good option for qualifying patients. These treatments are currently only available for those in or after their fourth line of therapy, but the anticipation is that they will be approved for earlier lines of therapy in the coming years.
- GPRC5D-targeting bispecific therapy, talquetamab, can also be used if the patient qualifies.
- Though not currently approved within the United States, belantamab-mafodotin (BLENREP) could be an option for these patients if reapproved, considering it has been a successful therapy for this population in the past.
Considerations for Next Therapy After Anti-BCMA Therapy
Dr. Adam Cohen spoke on treatment options for multiple myeloma patients after they were exposed to BCMA therapies.
Now is a remarkable time in multiple myeloma research, with six FDA approvals taking place over the span of the last three years, and several more to come in the pipeline. However, none of these therapies has yet been proven to be curative in late-line myeloma therapy, and more work needs to be done when it comes to achieving the best results possible for our relapsed/refractory myeloma patients.
Out of the past six approvals, five of those treatments share the same target, BCMA. This raises the key question of how to use these therapies sequentially if they share the same target, and if possible, what the optimal sequencing of those therapies can be in order to achieve the best response.
The problem is only going to get more complicated as earlier lines of approval for CAR-T cell therapies (ide-cel and cilta-cel) are approved because while this is promising, it also means that myeloma specialists are going to need to know the optimal next lines of therapy as/if patients relapse after these CAR-T cell therapies.
Dr. Cohen shares three different categories/options for the next line of therapy after a patient has been exposed to BCMA therapy:
- Different BCMA-Targeted Therapy
- Non BCMA-Targeted, T-Cell Engaging Therapy
- A Non T-Cell Engaging Therapy
The myeloma research field has finally established some data in terms of how to best sequence the new immunotherapies, something that both physicians and patients alike have been waiting for. Larger patient populations are necessary in order to solidify these findings.
There also remains little to no data in other key research areas and unfortunately no concrete answers yet regarding the best sequence or finding the most effective therapy combinations.
When thinking about best sequencing BCMA therapies, BCMA expression must be an important part of the conversation. Temporary BCMA expression loss usually occurs within patients after anti-BCMA therapies, and in very rare occasions, patients lose the ability to express BCMA permanently.
Using A Different BCMA-Targeted Therapy as Next Line of Treatment
Dr. Cohen reviewed common questions he has heard from providers (and answers) in his presentation:
Question: My patient has frozen T-cells left over. Can I treat them with the same product of CAR-T therapy that they just received?
Answer: Unfortunately, no; this theory has been tried several times and it has not been proven to be successful.
Question: After my patient receives one type of CAR-T cell product (i.e. cita-cel) could I treat them with a different CAR-T product (i.e. ide-cel) after relapse?
Answer: There is limited data on this subject. A clinical trial with limited numbers in China showed success from a non-approved CAR-T (CT103A phase 1) in which four of the 18 patients had previously received CAR-T therapy; all of them did well in the new clinical trial. This is probably not the ideal option and other therapies should be considered.
Question: Can I give a BCMA-directed CAR-T therapy after my patient has received a bispecific antibody or other form of BCMA-directed treatment?
Answer: Yes, though you can expect a shorter response duration in those patients. However, that isn't to say that the treatment will not be effective.
Question: Can I give a BCMA-directed bispecific antibody therapy after my patient has received a CAR-T or other form of BCMA-directed treatment?
Answer: Yes, the response rates are relatively similar between previously BCMA-exposed and BCMA-naive patients who received a bispecific antibody therapy after CAR-T or BLENREP. The duration of the response also is similar between these two populations.
Using Non-BCMA T-Cell Engaging Therapies As Next Line of Treatment
FDA-approved talquetamab, which targets GPRC5D, might be a great option for myeloma patients with previous anti-BCMA therapy exposure. You can learn more about talquetamab here: Talquetamab Approval in Myeloma (HealthTree). There are also CAR-T products in the clinical trial pipeline that target GPRC5D and could become an option.
Another option could be cevostamab, a bispecific antibody therapy targeting FcRH5. While still in clinical trials, its results have been promising, especially the duration of response experienced in patients who have stopped therapy but still continue to see results. This is discussed in more detail here: Cevostamab Bispecific Study (HealthTree).
Using Non-T-Cell Engaging Therapies As Next Line of Treatment
Non T-cell Engaging Therapies can be a great option for the next line of therapy in patients who have received anti-BCMA treatment.
These therapies could include:
- revisiting a new combo of previously used drugs in triplet or quadruplet
- salvage stem cell transplant
- combinations with Venetoclax for patients with 11;14 myeloma patients
- combinations with XPOVIO (selinexor)
- CELLMoDS (still in clinical trials) such as iberdomide or mezigdomide
- clinical trials
Conclusion
Though emerging myeloma research results are extremely promising and exciting, problems (such as how to best sequence or determine the best next line of therapy) arise. Continue to stay informed about emerging changes and developments as the myeloma treatment field continues to evolve and adapt. Staying up to date with a myeloma specialist on your team will be crucial for refining the best treatment approaches in the future.
ASH 2023 Resources
Would you like to watch ASH 2023 myeloma research interviews from the investigators themselves? Click "ASH 2023" here: HealthTree University Conference Coverage
To read other ASH 2023 articles, click here: HealthTree 2023 ASH Articles
I had a front-row seat for an educational seminar at ASH in which three specialists took a new look at current evidence that reflects best practices for relapsed and refractory multiple myeloma patient treatments.
Throughout the program, the presenters focused on three areas in which relapsed and refractory outcomes for multiple myeloma patients can improved:
- A rational approach to functional high-risk patients
- Considerations for the next therapy after anti-CD38 monoclonal antibodies used as first-line
- Options at the time of relapse after anti-BCMA therapy
Dr. Francesa Gay, MD, PhD began the session by discussing functional high-risk multiple myeloma.
Functional High-Risk Myeloma Patients
Functional high-risk patients can be defined as those who are not identified as high-risk at original diagnosis, but after standard-of-care treatments, relapse faster than the average myeloma patient, often within 12-18 months of their optimal initial therapy.
These patients can be treated with standard treatments such as immunomodulatory agents, proteasome inhibitors, and monoclonal antibodies. Other treatment options include novel therapies such as CAR-T cells, bispecific antibodies, and antibody-drug conjugates.
The table below shows articles or papers that dive into this issue. All of these tests were done on patients using, newer, standard-of-care treatments. However, the rate of earlier relapse ranges from 10-40%.
Despite the different reports and different treatments, the median overall survival for functional high-risk patients is two years. This is significantly inferior to the overall survival of those with standard myeloma that are often living over a decade.
There is a high medical need to find successful treatments or treatment sequencing for these patients as their post-relapse survival rates have not improved since 2005, despite the novel therapies that are being developed and approved at a rapid pace.
The problem is identifying the functional high-risk myeloma patients before they relapse, something quite difficult to do considering most patients aren’t classified as functional high-risk until they are relapsing early, and 10-20% of the myeloma patients who are functionally high risk have no classic high-risk indications (such as high tumor burden, high-risk mutations, or advanced ISS staging).
One predictor for identifying functionally high-risk patients lies in the quality of response that they have to their standard-of-care treatments. Those with suboptimal responses, for example not achieving VGPR or CR after their induction therapy, are more likely to be classified as high-risk.
It’s also important to note that patients can change their risk status. In fact, in one highlighted study 54% of patients changed their risk status after 9 months.
How can functionally high-risk patients be managed when they relapse “early”?
The majority of these patients are refractory to previous treatments. Refractory status can be defined as a disease that becomes nonresponsive or progressive on therapy within 60 days of the last treatment. Patients usually achieve minimal responses to these therapies.
This makes treating these patients more difficult as they have fewer options available to them that can effectively fight their myeloma. A myeloma specialist can help you navigate your care when considering the various options for myeloma treatment as detailed at this link: Myeloma Treatment Options (HealthTree)
It makes the most sense to treat functional high-risk myeloma patients after relapse with a change in drug class. An example of a possible treatment algorithm for functional high-risk patients can be seen below:
Dr. Gay presented several options for clinicians in charge of treating patients. There are options for first relapse options in lenalidomide naive patients: proteasome inhibitors backbone, or early immunotherapy.
This is a moment to stop and reinforce the lifesaving importance of having a myeloma specialist on your team. They are in tune with the newest research and can help you make key decisions in your treatment sequencing that can prolong your life and significantly improve the quality. Check out our specialist directory here: Multiple Myeloma Specialist Directory
Considerations for Next Therapy After Anti-CD38 Monoclonal Antibodies Used As First-Line
Dr. Monique Hartley-Brown's focus was improving treatment for relapsed/refractory multiple myeloma patients after anti-CD38 therapy exposure in their first line of therapy.
As a reminder, CD38 is highly expressed on multiple myeloma cells, and functions as a receptor (adhesion molecule) that mediates immunosuppression. CD38 is expressed in the bone marrow microenvironment and is also expressed by immune cells, such as T-cells, NK cells, and more.
CD38 is therefore a critical target in multiple myeloma therapy, and anti-CD38 monoclonal antibodies used to treat myeloma are truly transforming newly diagnosed myeloma treatment. For more information on monoclonal antibody treatments for multiple myeloma, check them out here: Monoclonal Antibody Myeloma Treatments (HealthTree)
There are two anti-CD38 monoclonal antibodies that are currently FDA-approved for myeloma treatment, isatuximab and daratumamab. They work slightly differently from each other, and could possibly be valuable as complementary/alternative therapies to one another.
After the published GRIFFIN study (as seen below), several multiple myeloma specialists and even specialist centers have started to change their standard-of-care induction therapies for newly diagnosed multiple myeloma patients to include anti-CD38 therapies.
Even at this particular ASH conference, there was a lot of excitement and interest surrounding the findings of isatuximab and its ability to get many patients into MRD (minimal residual disease) negativity.
Other key clinical trials such as the MAIA trial and the Phase III trial PERSEUS (which was also presented with much anticipation at this ASH conference) have proven the effectiveness of adding an anti-CD38 monoclonal antibody as shown in the GRIFFIN study.
Many more clinical trials testing various versions of an induction quadrupled with an anti-CD38 monoclonal antibody are currently in the pipeline.
Because more patients are receiving anti-CD38 myeloma therapies upfront, the question remains of how/with which therapies to treat these patients when the disease begins to progress. What are viable and effective second and third line therapies for patients that are in this situation?
- A deferred stem cell transplant could be a great option for these patients. An upfront transplant doesn't offer any overall survival benefits, so "saving" the stem cell transplant for a further line of therapy instead of including it as a part of the induction/consolidation therapy might be the right answer for a selection of patients.
- Another option could be the use of selinexor, bortezomib and dexamethasone could be an option for a patient in this situation. Findings in the BOSTON trial showed this combination to be more successful than combining bortezomib and dexamethasone alone.
- BCMA-targeted therapies such as CAR-T therapy or bispecific antibodies like teclistimab or elranatamab could be a good option for qualifying patients. These treatments are currently only available for those in or after their fourth line of therapy, but the anticipation is that they will be approved for earlier lines of therapy in the coming years.
- GPRC5D-targeting bispecific therapy, talquetamab, can also be used if the patient qualifies.
- Though not currently approved within the United States, belantamab-mafodotin (BLENREP) could be an option for these patients if reapproved, considering it has been a successful therapy for this population in the past.
Considerations for Next Therapy After Anti-BCMA Therapy
Dr. Adam Cohen spoke on treatment options for multiple myeloma patients after they were exposed to BCMA therapies.
Now is a remarkable time in multiple myeloma research, with six FDA approvals taking place over the span of the last three years, and several more to come in the pipeline. However, none of these therapies has yet been proven to be curative in late-line myeloma therapy, and more work needs to be done when it comes to achieving the best results possible for our relapsed/refractory myeloma patients.
Out of the past six approvals, five of those treatments share the same target, BCMA. This raises the key question of how to use these therapies sequentially if they share the same target, and if possible, what the optimal sequencing of those therapies can be in order to achieve the best response.
The problem is only going to get more complicated as earlier lines of approval for CAR-T cell therapies (ide-cel and cilta-cel) are approved because while this is promising, it also means that myeloma specialists are going to need to know the optimal next lines of therapy as/if patients relapse after these CAR-T cell therapies.
Dr. Cohen shares three different categories/options for the next line of therapy after a patient has been exposed to BCMA therapy:
- Different BCMA-Targeted Therapy
- Non BCMA-Targeted, T-Cell Engaging Therapy
- A Non T-Cell Engaging Therapy
The myeloma research field has finally established some data in terms of how to best sequence the new immunotherapies, something that both physicians and patients alike have been waiting for. Larger patient populations are necessary in order to solidify these findings.
There also remains little to no data in other key research areas and unfortunately no concrete answers yet regarding the best sequence or finding the most effective therapy combinations.
When thinking about best sequencing BCMA therapies, BCMA expression must be an important part of the conversation. Temporary BCMA expression loss usually occurs within patients after anti-BCMA therapies, and in very rare occasions, patients lose the ability to express BCMA permanently.
Using A Different BCMA-Targeted Therapy as Next Line of Treatment
Dr. Cohen reviewed common questions he has heard from providers (and answers) in his presentation:
Question: My patient has frozen T-cells left over. Can I treat them with the same product of CAR-T therapy that they just received?
Answer: Unfortunately, no; this theory has been tried several times and it has not been proven to be successful.
Question: After my patient receives one type of CAR-T cell product (i.e. cita-cel) could I treat them with a different CAR-T product (i.e. ide-cel) after relapse?
Answer: There is limited data on this subject. A clinical trial with limited numbers in China showed success from a non-approved CAR-T (CT103A phase 1) in which four of the 18 patients had previously received CAR-T therapy; all of them did well in the new clinical trial. This is probably not the ideal option and other therapies should be considered.
Question: Can I give a BCMA-directed CAR-T therapy after my patient has received a bispecific antibody or other form of BCMA-directed treatment?
Answer: Yes, though you can expect a shorter response duration in those patients. However, that isn't to say that the treatment will not be effective.
Question: Can I give a BCMA-directed bispecific antibody therapy after my patient has received a CAR-T or other form of BCMA-directed treatment?
Answer: Yes, the response rates are relatively similar between previously BCMA-exposed and BCMA-naive patients who received a bispecific antibody therapy after CAR-T or BLENREP. The duration of the response also is similar between these two populations.
Using Non-BCMA T-Cell Engaging Therapies As Next Line of Treatment
FDA-approved talquetamab, which targets GPRC5D, might be a great option for myeloma patients with previous anti-BCMA therapy exposure. You can learn more about talquetamab here: Talquetamab Approval in Myeloma (HealthTree). There are also CAR-T products in the clinical trial pipeline that target GPRC5D and could become an option.
Another option could be cevostamab, a bispecific antibody therapy targeting FcRH5. While still in clinical trials, its results have been promising, especially the duration of response experienced in patients who have stopped therapy but still continue to see results. This is discussed in more detail here: Cevostamab Bispecific Study (HealthTree).
Using Non-T-Cell Engaging Therapies As Next Line of Treatment
Non T-cell Engaging Therapies can be a great option for the next line of therapy in patients who have received anti-BCMA treatment.
These therapies could include:
- revisiting a new combo of previously used drugs in triplet or quadruplet
- salvage stem cell transplant
- combinations with Venetoclax for patients with 11;14 myeloma patients
- combinations with XPOVIO (selinexor)
- CELLMoDS (still in clinical trials) such as iberdomide or mezigdomide
- clinical trials
Conclusion
Though emerging myeloma research results are extremely promising and exciting, problems (such as how to best sequence or determine the best next line of therapy) arise. Continue to stay informed about emerging changes and developments as the myeloma treatment field continues to evolve and adapt. Staying up to date with a myeloma specialist on your team will be crucial for refining the best treatment approaches in the future.
ASH 2023 Resources
Would you like to watch ASH 2023 myeloma research interviews from the investigators themselves? Click "ASH 2023" here: HealthTree University Conference Coverage
To read other ASH 2023 articles, click here: HealthTree 2023 ASH Articles

about the author
Beth Travis
Beth is a licensed Physical Therapist that truly believes in the benefits of exercise. Mother of two, a myeloma patient and advocate with a love of learning, healthy lifestyles and food adventures.





Trending Articles



Upcoming Events



Get the Latest Multiple Myeloma Updates, Delivered to You.
By subscribing to the HealthTree newsletter, you'll receive the latest research, treatment updates, and expert insights to help you navigate your health.
Together we care.
Together we cure.