ASH 2021: One Step Closer to Chemo Free Living?

Achieving a prolonged minimal residual disease (MRD) standard after consolidation may raise hope for a chemo-free future for patients who respond well to therapy and liberate them from maintenance according by Dr. Luciano Costa, from the University of Alabama at Birmingham, at the recent annual American Society of Hematology meeting.
The MASTER trial proposed modifying post autologous stem cell transplant (ASCT) consolidation and maintenance; to make them dependent on the depth of response achieved, with up to 80% of patients qualifying for treatment-free observation.
Patients who achieved MRD negativity entered treatment-free observation (known as MRD-SURE) with continued MRD monitoring for recurrence. Those who did not become MRD-SURE entered lenalidomide maintenance.
Separating newly diagnosed (NDMM), transplant-eligible patients according to their number of high-risk cytogenetic features (HRCA), ranging from zero to two or more, all patients received induction Dara-KRd (daratumumab, carfilzomib, lenalidomide, dexamethasone), followed by transplant. This combination resulted in an unprecedented depth of response in NDMM patients, as measured by minimal residual disease MRD status.
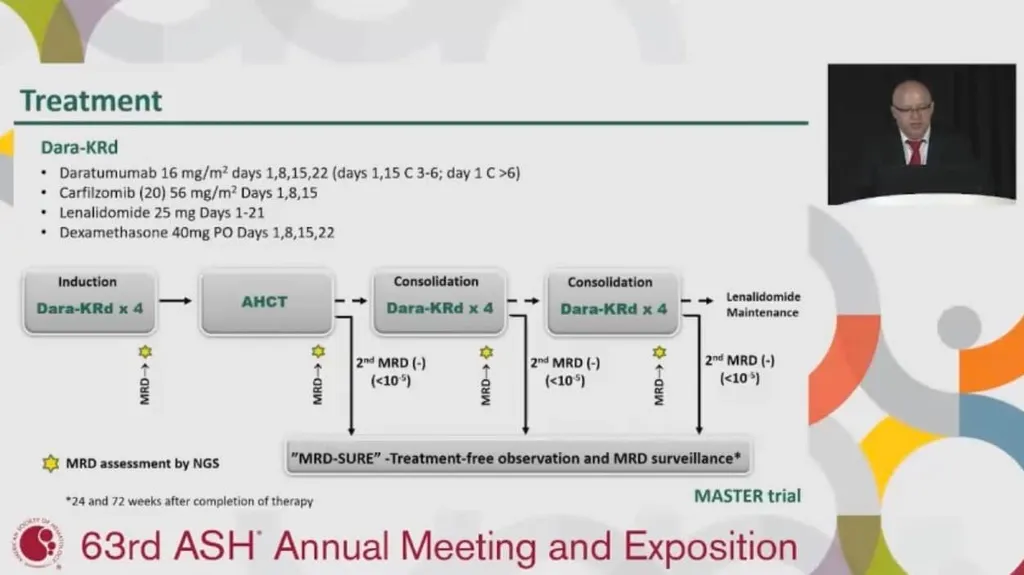
Decisions about modification and/or possible cessation of therapy was dependent upon the depth of response, as measured by MRD. Following transplant, patients received Dara-KRd as consolidation therapy.
The number of cycles of consolidation therapy patients received was dictated by their MRD status, was checked frequently, which was a novel approach. Patients continued on consolidation until they tested MRD negative (at 10-5) on two consecutive tests or until the consolidation phase ended (eight cycles of Dara-KRd).
Dr. Costa’s team sought to define the most appropriate post-ASCT consolidation therapy. Overall, 71% of patients achieved MRD-SURE status and progression free survival rates were 91%, 97%, 58% for patients with 0, 1 and 2+ high risk features, respectively.
The MASTER trial has been, and continues to be, a treasure trove of data for the newly diagnosed myeloma patient. Certainly, the DARA-KRD induction, followed by ASCT, has shown an unprecedented depth of response.
MRD surveillance for the MRD-SURE patient represents a new possibility that inspires continued trials. While the MASTER data does not qualify observation only as a current standard of care, it does offer hope that there may be a maintenance free future for a significant percentage of newly diagnosed myeloma patients.
Will there ever be time when I can be treatment free or will I always be on some form of chemotherapy? This dilemma is on the mind of every myeloma patient may soon become less of one for patients who respond well to treatment.
Achieving a prolonged minimal residual disease (MRD) standard after consolidation may raise hope for a chemo-free future for patients who respond well to therapy and liberate them from maintenance according by Dr. Luciano Costa, from the University of Alabama at Birmingham, at the recent annual American Society of Hematology meeting.
The MASTER trial proposed modifying post autologous stem cell transplant (ASCT) consolidation and maintenance; to make them dependent on the depth of response achieved, with up to 80% of patients qualifying for treatment-free observation.
Patients who achieved MRD negativity entered treatment-free observation (known as MRD-SURE) with continued MRD monitoring for recurrence. Those who did not become MRD-SURE entered lenalidomide maintenance.
Separating newly diagnosed (NDMM), transplant-eligible patients according to their number of high-risk cytogenetic features (HRCA), ranging from zero to two or more, all patients received induction Dara-KRd (daratumumab, carfilzomib, lenalidomide, dexamethasone), followed by transplant. This combination resulted in an unprecedented depth of response in NDMM patients, as measured by minimal residual disease MRD status.
Decisions about modification and/or possible cessation of therapy was dependent upon the depth of response, as measured by MRD. Following transplant, patients received Dara-KRd as consolidation therapy.
The number of cycles of consolidation therapy patients received was dictated by their MRD status, was checked frequently, which was a novel approach. Patients continued on consolidation until they tested MRD negative (at 10-5) on two consecutive tests or until the consolidation phase ended (eight cycles of Dara-KRd).
Dr. Costa’s team sought to define the most appropriate post-ASCT consolidation therapy. Overall, 71% of patients achieved MRD-SURE status and progression free survival rates were 91%, 97%, 58% for patients with 0, 1 and 2+ high risk features, respectively.
The MASTER trial has been, and continues to be, a treasure trove of data for the newly diagnosed myeloma patient. Certainly, the DARA-KRD induction, followed by ASCT, has shown an unprecedented depth of response.
MRD surveillance for the MRD-SURE patient represents a new possibility that inspires continued trials. While the MASTER data does not qualify observation only as a current standard of care, it does offer hope that there may be a maintenance free future for a significant percentage of newly diagnosed myeloma patients.
Will there ever be time when I can be treatment free or will I always be on some form of chemotherapy? This dilemma is on the mind of every myeloma patient may soon become less of one for patients who respond well to treatment.

about the author
Kyle Colvin, MD
“As a physician, I figured I may have a unique perspective on the disease, as well as a knowledge base and the time to help patients understand the disease course and treatment options. I figure that I should give back to those in need since my life has been incredibly fortunate, even with this disease.”
More on Conferences






Trending Articles



Upcoming Events




Get the Latest Multiple Myeloma Updates, Delivered to You.
By subscribing to the HealthTree newsletter, you'll receive the latest research, treatment updates, and expert insights to help you navigate your health.
Together we care.
Together we cure.