ASH 2018: High Risk and "Double Hit" Myeloma
The Friday symposium sessions are some of the best at ASH, even though they are not an official part of the American Society of Hematology session.
Dr. Keith Stuart of the Mayo Clinic spoke at a morning session on the topic of high risk myeloma, with some key points. He said that while treatment is improving for myeloma patients with the advent of a growing number of combination therapies, there are still 25% of myeloma patients with high-risk disease who live less than 3 years. Patients with the genetic myeloma features of 4;14, 14;16 and del17 are of the highest risk.
He noted that risk is categorized into International Staging System "stages."
ISS Stage 1 patients:
- Normal albumin levels
- No high risk genetics features
- Normal LDH levels
ISS Stage 2 patients:
- High LDH level OR a high risk feature
- High Beta-2 Microglobulin levels
ISS Stage 3 patients:
- All other possible combinations
He mentioned that while normal patients can do well on typical treatment (such as induction with Revlimid/Velcade/Dex, then a stem cell transplant and lenalidomide maintenance therapy), high-risk patients will still want to have a transplant but use a proteasome inhibitor such as carfilzomib or bortezomib on an ongoing basis until their disease progresses.
For patients with "Double Hit" myeloma, (explained below) he suggested that a stronger induction therapy using Revlimid/carfilzomib/dex may be used instead of Rev/Velcade/dex.
For patients with the translocation of 4;14 included 15% of the total myeloma patient population. These patients often have an IgA type of myeloma. Frequently, they also have an accompanying del17p. For these patients he also suggested extended proteasome inhibitor maintenance.
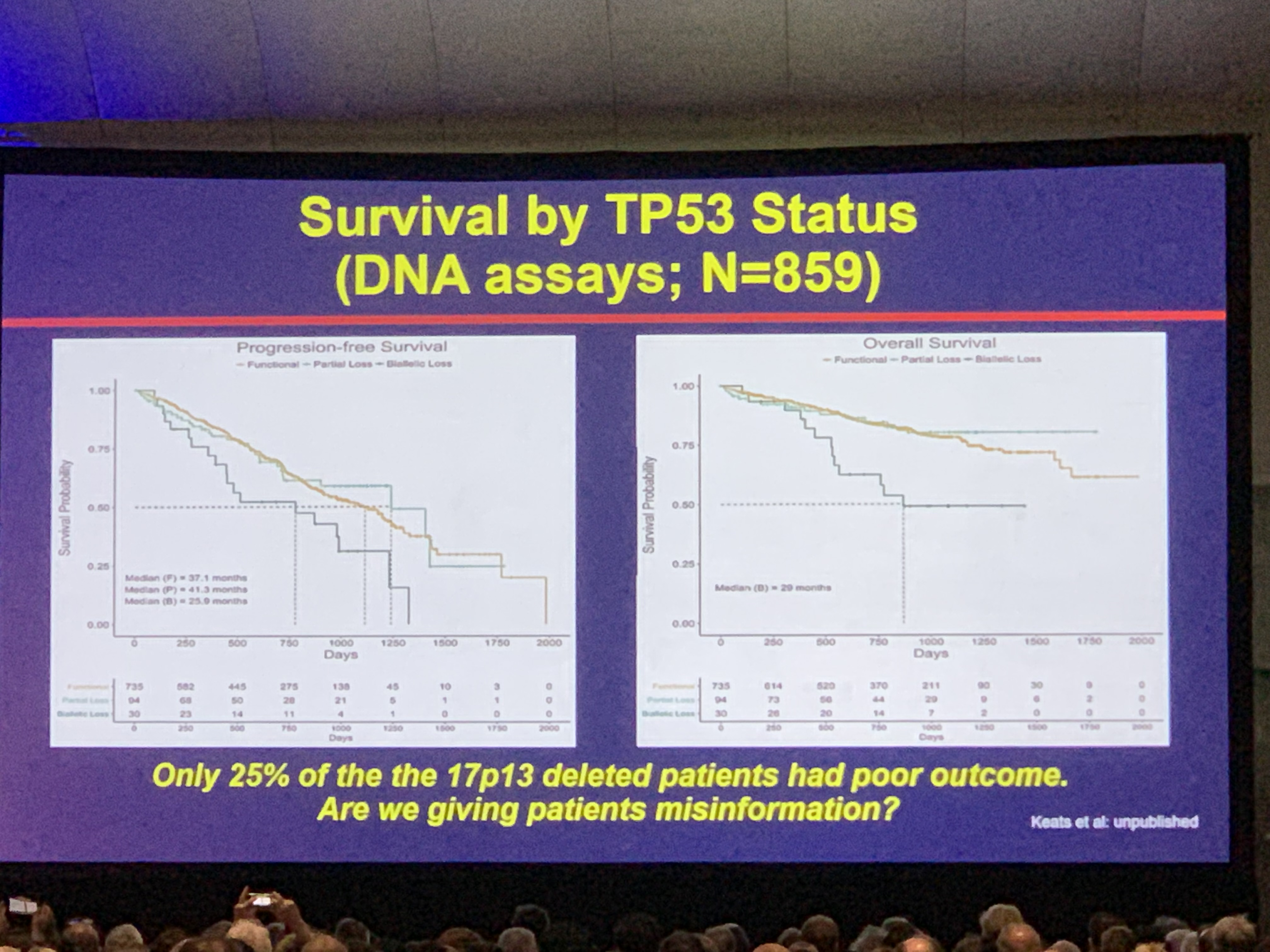
Dr. Stuart cited the CoMMpaSS study genomic data of 1150 patients. Amazing analysis work by Jonathan Keats at TGEN found that in patients who lost only one of the copies of 17p on their myeloma cells, their myeloma did NOT behave as high-risk. In patients who lost both copies of 17p, their myeloma DID behave as high-risk. Dr. Stuart stressed this important finding. "We are telling 75% of our del17p patients they are high risk when they are not."
Importantly, he also cited work by Dr. Gareth Morgan and Dr. Brian Walker of UAMS showing that patients who had the 1q gain was ONLY high risk when they had 4 copies of the chromosome, but not 3 copies of the chromosomes.
Either one of these (double copy losses of del17p or 4 copies of the 1q gain) is called "Double Hit" myeloma - as a new disease segment for extremely high risk disease in newly diagnosed multiple myeloma patients. This involves 6.1% of the total myeloma patient population.
This information is not available on the most commonly run test in myeloma - the FISH test. Further and deeper genomic testing needs to be done for these patients.
Also important is the percentage of cells with the genetic mutation. For example, a low percent of del17p cells (like 5%) is much less aggressive than a higher percentage of cells (like 80%).
In summary, it is key for myeloma patients to better understand their disease if they have high risk features to understand how they should be treated.
The Friday symposium sessions are some of the best at ASH, even though they are not an official part of the American Society of Hematology session.
Dr. Keith Stuart of the Mayo Clinic spoke at a morning session on the topic of high risk myeloma, with some key points. He said that while treatment is improving for myeloma patients with the advent of a growing number of combination therapies, there are still 25% of myeloma patients with high-risk disease who live less than 3 years. Patients with the genetic myeloma features of 4;14, 14;16 and del17 are of the highest risk.
He noted that risk is categorized into International Staging System "stages."
ISS Stage 1 patients:
- Normal albumin levels
- No high risk genetics features
- Normal LDH levels
ISS Stage 2 patients:
- High LDH level OR a high risk feature
- High Beta-2 Microglobulin levels
ISS Stage 3 patients:
- All other possible combinations
He mentioned that while normal patients can do well on typical treatment (such as induction with Revlimid/Velcade/Dex, then a stem cell transplant and lenalidomide maintenance therapy), high-risk patients will still want to have a transplant but use a proteasome inhibitor such as carfilzomib or bortezomib on an ongoing basis until their disease progresses.
For patients with "Double Hit" myeloma, (explained below) he suggested that a stronger induction therapy using Revlimid/carfilzomib/dex may be used instead of Rev/Velcade/dex.
For patients with the translocation of 4;14 included 15% of the total myeloma patient population. These patients often have an IgA type of myeloma. Frequently, they also have an accompanying del17p. For these patients he also suggested extended proteasome inhibitor maintenance.
Dr. Stuart cited the CoMMpaSS study genomic data of 1150 patients. Amazing analysis work by Jonathan Keats at TGEN found that in patients who lost only one of the copies of 17p on their myeloma cells, their myeloma did NOT behave as high-risk. In patients who lost both copies of 17p, their myeloma DID behave as high-risk. Dr. Stuart stressed this important finding. "We are telling 75% of our del17p patients they are high risk when they are not."
Importantly, he also cited work by Dr. Gareth Morgan and Dr. Brian Walker of UAMS showing that patients who had the 1q gain was ONLY high risk when they had 4 copies of the chromosome, but not 3 copies of the chromosomes.
Either one of these (double copy losses of del17p or 4 copies of the 1q gain) is called "Double Hit" myeloma - as a new disease segment for extremely high risk disease in newly diagnosed multiple myeloma patients. This involves 6.1% of the total myeloma patient population.
This information is not available on the most commonly run test in myeloma - the FISH test. Further and deeper genomic testing needs to be done for these patients.
Also important is the percentage of cells with the genetic mutation. For example, a low percent of del17p cells (like 5%) is much less aggressive than a higher percentage of cells (like 80%).
In summary, it is key for myeloma patients to better understand their disease if they have high risk features to understand how they should be treated.

about the author
Jennifer Ahlstrom
Myeloma survivor, patient advocate, wife, mom of 6. Believer that patients can contribute to cures by joining HealthTree Cure Hub and joining clinical research. Founder and CEO of HealthTree Foundation.
More on Treatment Advances






Trending Articles







Get the Latest Multiple Myeloma Updates, Delivered to You.
By subscribing to the HealthTree newsletter, you'll receive the latest research, treatment updates, and expert insights to help you navigate your health.
Together we care.
Together we cure.