

Lenalidomide maintenance was then given in all arms.
The study included a total of 1503 patients under the age of 65 with 618 of those patients being split into a VMP (203 patients), single transplant (208 patients) or tandem transplant arm (207 patients). The study objective looked at progression-free survival.
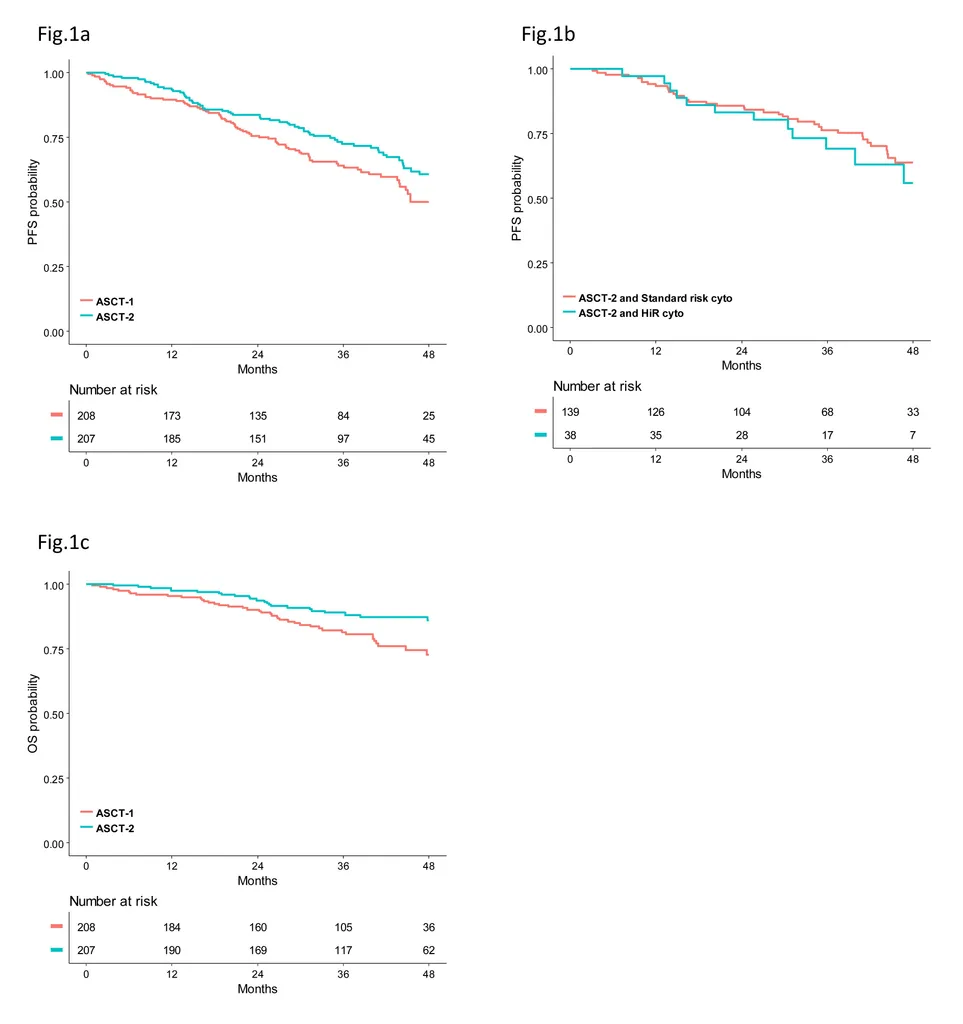
The study included a large number of high risk patients (as defined by t(4;14), t(14;16), deletion 17p, deletion 1p or gain of 1q status) in the single or tandem transplant arms. The median follow-up was 38 months.
The three-year estimate of progression free survival was 73% for the tandem transplant group vs. 64% for the single transplant group, which represented a 30% reduced risk. (Figure 1a)
Overall survival was prolonged with the tandem transplant (89%) vs. the single transplant (82%). (Figure 1c)
For high risk patients, the progression free survival was also extended, helping them receive similar outcomes as standard risk patients. (Figure 1b)
Europe as a whole does not have access to some treatments and combination therapies typically used in the United States. With fewer drugs approved, they were able to utilize tandem transplant as an effective tool to prolong progression free and overall survival, especially those with high risk disease. The addition of bortezomib in the tandem transplant arm also assisted high risk patients (especially those with del17p) in obtaining better outcomes.
 In a separate paper, German researchers also studied 1115 patients who underwent single vs. tandem transplants. They found higher progression free survival and overall survival for patients who did not have deep responses after the first transplant. They did not find advantage of a second transplant for patients who achieved a complete response after the first transplant. This emphasizes the point that high risk patients need to obtain deep responses and continue those deep responses for prolonged periods of time. Achieving a complete response is more critical to these patients.
It will be fascinating to see how the addition of newer agents like monoclonal antibodies, next generation proteasome inhibitors like ixazomib and carfilzomib or other therapies could further increase patient outcomes as they are added to single or tandem transplant and if we can achieve even better outcomes overall.
In a separate paper, German researchers also studied 1115 patients who underwent single vs. tandem transplants. They found higher progression free survival and overall survival for patients who did not have deep responses after the first transplant. They did not find advantage of a second transplant for patients who achieved a complete response after the first transplant. This emphasizes the point that high risk patients need to obtain deep responses and continue those deep responses for prolonged periods of time. Achieving a complete response is more critical to these patients.
It will be fascinating to see how the addition of newer agents like monoclonal antibodies, next generation proteasome inhibitors like ixazomib and carfilzomib or other therapies could further increase patient outcomes as they are added to single or tandem transplant and if we can achieve even better outcomes overall.
ASH 2017: Tandem Transplant Better than Single Transplant in European Studies, Especially for High Risk Patients

Stem cell transplant continues to be the single most effective therapy in the treatment of multiple myeloma, even in the age of newer treatments. Italian and Dutch researchers presented data at ASH on Sunday showing that tandem transplant was better than single transplant when using an induction therapy of bortezomib/cyclophospamide/dex as induction therapy for newly diagnosed myeloma patients who then went on to one of three options:
- Treatment with bortezomib/melphalan/prednisone (VMP) for four 42-day cycles OR
- Single autologous transplant OR
- Second autologous transplant
Stem cell transplant continues to be the single most effective therapy in the treatment of multiple myeloma, even in the age of newer treatments. Italian and Dutch researchers presented data at ASH on Sunday showing that tandem transplant was better than single transplant when using an induction therapy of bortezomib/cyclophospamide/dex as induction therapy for newly diagnosed myeloma patients who then went on to one of three options:
- Treatment with bortezomib/melphalan/prednisone (VMP) for four 42-day cycles OR
- Single autologous transplant OR
- Second autologous transplant
Lenalidomide maintenance was then given in all arms.
The study included a total of 1503 patients under the age of 65 with 618 of those patients being split into a VMP (203 patients), single transplant (208 patients) or tandem transplant arm (207 patients). The study objective looked at progression-free survival. The study included a large number of high risk patients (as defined by t(4;14), t(14;16), deletion 17p, deletion 1p or gain of 1q status) in the single or tandem transplant arms. The median follow-up was 38 months. The three-year estimate of progression free survival was 73% for the tandem transplant group vs. 64% for the single transplant group, which represented a 30% reduced risk. (Figure 1a) Overall survival was prolonged with the tandem transplant (89%) vs. the single transplant (82%). (Figure 1c) For high risk patients, the progression free survival was also extended, helping them receive similar outcomes as standard risk patients. (Figure 1b) Europe as a whole does not have access to some treatments and combination therapies typically used in the United States. With fewer drugs approved, they were able to utilize tandem transplant as an effective tool to prolong progression free and overall survival, especially those with high risk disease. The addition of bortezomib in the tandem transplant arm also assisted high risk patients (especially those with del17p) in obtaining better outcomes.
In a separate paper, German researchers also studied 1115 patients who underwent single vs. tandem transplants. They found higher progression free survival and overall survival for patients who did not have deep responses after the first transplant. They did not find advantage of a second transplant for patients who achieved a complete response after the first transplant. This emphasizes the point that high risk patients need to obtain deep responses and continue those deep responses for prolonged periods of time. Achieving a complete response is more critical to these patients.
It will be fascinating to see how the addition of newer agents like monoclonal antibodies, next generation proteasome inhibitors like ixazomib and carfilzomib or other therapies could further increase patient outcomes as they are added to single or tandem transplant and if we can achieve even better outcomes overall.

about the author
Jennifer Ahlstrom
Myeloma survivor, patient advocate, wife, mom of 6. Believer that patients can contribute to cures by joining HealthTree Cure Hub and joining clinical research. Founder and CEO of HealthTree Foundation.
More on Treatment Advances




Trending Articles






Get the Latest Multiple Myeloma Updates, Delivered to You.
By subscribing to the HealthTree newsletter, you'll receive the latest research, treatment updates, and expert insights to help you navigate your health.
Education
News Articles Patient Guides My Journal University Expert Webinars Find a Specialist HealthTree PodcastCommunity
Connect Coach Moves All Events Community Support Groups Black Myeloma Health Resources in SpanishCure Hub
HealthTree Cure Hub Find Side Effects Solutions See Tracked Labs Connect Medical Records Treatment Options Twin Machine Clinical Trial FinderFollow Us




HealthTree Foundation is a qualified 501(c)(3) tax-exempt organization.
Copyright © 2025 HealthTree Foundation. All rights reserved.
Tax ID 45-5354811