Precision Medicine for Multiple Myeloma

The Myeloma Crowd by HealthTree has reiterated time and again that multiple myeloma is a heterogeneous disease (i.e. not all myeloma is the same). In practice, this means that two different patients with similar clinical characteristics may not react the same when treated with the same regimen. This is one of the reasons why myeloma is such a difficult disease to stabilize and treat, even with the ever-increasing list of novel treatment options that have become available to us. The ‘Holy Grail’ is to design a treatment plan that is specifically defined to treat our very own specific disease characteristics and markers.
A recent article in the Journal of Clinical Oncology – Precision Oncology summarizes the results of efforts by a team of researchers from Fred Hutch/University of Washington Cancer Consortium. Their work shows that:
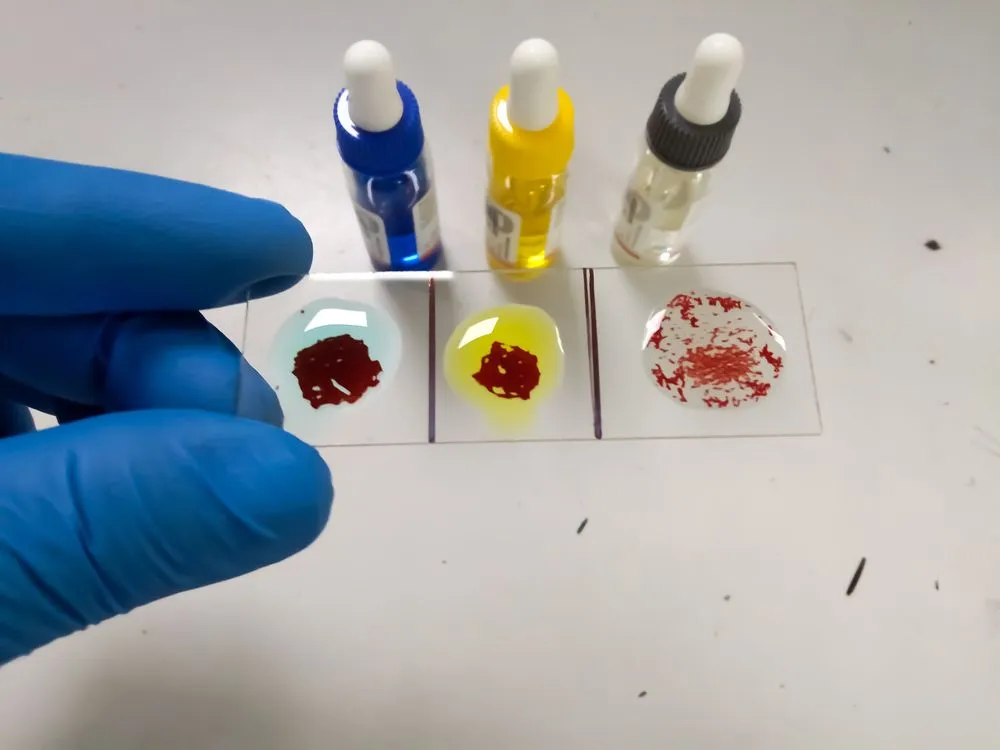
‘… ex vivo drug testing is a feasible strategy for informing real time therapeutic decisions for MM patients.’
Ex vivo means that the drug testing is being done in the lab, as opposed to trying out drugs on sick patients.
‘The goal of this clinical trial was to use ex vivo, high-throughput screening (HTS) of 170 compounds to predict response among patients with relapsed or refractory MM and inform the next treatment decisions. Additionally, we integrated HTS with multi-omic analysis to uncover novel associations between in vitro drug sensitivity and gene expression and mutation profiles.’ [emphasis added].
[Multiomics, multi-omics, integrative omics, 'pan-omics' is a biological analysis approach in which the data sets are multiple "omes", such as the genome, proteome, transcriptome, epigenome, metabolome, and microbiome; in other words, the use of multiple omics technologies to study life in a concerted way. By combining these "omes", scientists can analyze complex biological big data to find novel associations between biological entities, pinpoint relevant biomarkers and build elaborate markers of disease and physiology.]
The trial recruited 25 patients whose myeloma had relapsed after at least 3 prior lines of therapy. Fresh plasma cells from bone marrow or localized tumor growths (extramedullary plasmacytomas) were collected from each patient with the intent to collect at least 600,000 myeloma cells for lab testing. Nine patients did not yield the targeted number of plasma cells and were excluded from this particular study.
The harvested cells were divided over 384 culture plates and tested against a library of 170 drugs for potential treatment, made up of both drugs currently FDA approved as well as some experimental drugs, using a high throughput screen [HTS] lab assay. Of note is that the 170 drugs were tested at 8 different concentrations. The cells were incubated for three days, and samples were tested for cell viability and inhibition of cell growth for a given compound. In addition, ‘Targeted next-generation sequencing was performed on plasma cell-free DNA from all patients who underwent HTS. RNA and whole-exome sequencing [a type of genetic sequencing increasingly used to understand what may be causing symptoms or a disease] of bone marrow plasma cells were performed on eight and seven patients, respectively’.
Let’s digress here for a few lines. All of us tend to be aware of several handfuls of drugs used in the treatment for myeloma and may now ask the question “170 drugs for myeloma ? Where do they come from ?” This question is answered in a press release from Fred Hutch. The body of this press statement shows a chart with all 170 listed by therapeutic category (e.g., proteasome inhibitors) and you are bound to find drugs and drug categories you may have not yet heard of.
The results of this massive study for each patient were received in 5 days from the time that plasma cells were collected from the patients. The results for the 16 patients tested can be summarized as follows:
- 'A list of recommended drugs was provided to the patients’ oncologists and treatment choice was left to their discretion. FDA approval status, insurance coverage, prior treatment history, known side effect profiles, and patient preference were all factors considered in decision making. Combination therapies with drugs not included in the screening panel were allowed, and FDA approved drug doses were used regardless of HTS outcomes.’
- '13 of the 16 HTS patients received treatments that were recommended by HTS.’
- '92% of those patients achieved at least stable disease, with 31% partial responses and 15% very good partial responses. No complete responses were observed in this heavily pretreated group of patients.’
- ‘ … this work uncovered novel associations between genomic profiling data and drug sensitivity.’
- ‘The expression of 105 genes and mutations in 12 genes correlated with in vitro cytotoxicity.’
The researchers have also outlined plans for future development. They are expected to include a smaller number of drugs in their testing library so that fewer malignant cells need to be harvested which will increase the number of patients that may/will benefit from this technology. In addition, the larger patient population will allow the validation of the assay’s ability to predict clinical response. ‘Ongoing studies will also test therapeutic combinations, to reduce the opportunity for acquired drug resistance.’
Further fine-tuning of this technology may/will be of significant importance to us in the future, especially at time of relapse, when a drug treatment plan can be defined that is very specific to our specific individual clinical need. Something else to give us hope for the future.
The Myeloma Crowd by HealthTree has reiterated time and again that multiple myeloma is a heterogeneous disease (i.e. not all myeloma is the same). In practice, this means that two different patients with similar clinical characteristics may not react the same when treated with the same regimen. This is one of the reasons why myeloma is such a difficult disease to stabilize and treat, even with the ever-increasing list of novel treatment options that have become available to us. The ‘Holy Grail’ is to design a treatment plan that is specifically defined to treat our very own specific disease characteristics and markers.
A recent article in the Journal of Clinical Oncology – Precision Oncology summarizes the results of efforts by a team of researchers from Fred Hutch/University of Washington Cancer Consortium. Their work shows that:
‘… ex vivo drug testing is a feasible strategy for informing real time therapeutic decisions for MM patients.’
Ex vivo means that the drug testing is being done in the lab, as opposed to trying out drugs on sick patients.
‘The goal of this clinical trial was to use ex vivo, high-throughput screening (HTS) of 170 compounds to predict response among patients with relapsed or refractory MM and inform the next treatment decisions. Additionally, we integrated HTS with multi-omic analysis to uncover novel associations between in vitro drug sensitivity and gene expression and mutation profiles.’ [emphasis added].
[Multiomics, multi-omics, integrative omics, 'pan-omics' is a biological analysis approach in which the data sets are multiple "omes", such as the genome, proteome, transcriptome, epigenome, metabolome, and microbiome; in other words, the use of multiple omics technologies to study life in a concerted way. By combining these "omes", scientists can analyze complex biological big data to find novel associations between biological entities, pinpoint relevant biomarkers and build elaborate markers of disease and physiology.]
The trial recruited 25 patients whose myeloma had relapsed after at least 3 prior lines of therapy. Fresh plasma cells from bone marrow or localized tumor growths (extramedullary plasmacytomas) were collected from each patient with the intent to collect at least 600,000 myeloma cells for lab testing. Nine patients did not yield the targeted number of plasma cells and were excluded from this particular study.
The harvested cells were divided over 384 culture plates and tested against a library of 170 drugs for potential treatment, made up of both drugs currently FDA approved as well as some experimental drugs, using a high throughput screen [HTS] lab assay. Of note is that the 170 drugs were tested at 8 different concentrations. The cells were incubated for three days, and samples were tested for cell viability and inhibition of cell growth for a given compound. In addition, ‘Targeted next-generation sequencing was performed on plasma cell-free DNA from all patients who underwent HTS. RNA and whole-exome sequencing [a type of genetic sequencing increasingly used to understand what may be causing symptoms or a disease] of bone marrow plasma cells were performed on eight and seven patients, respectively’.
Let’s digress here for a few lines. All of us tend to be aware of several handfuls of drugs used in the treatment for myeloma and may now ask the question “170 drugs for myeloma ? Where do they come from ?” This question is answered in a press release from Fred Hutch. The body of this press statement shows a chart with all 170 listed by therapeutic category (e.g., proteasome inhibitors) and you are bound to find drugs and drug categories you may have not yet heard of.
The results of this massive study for each patient were received in 5 days from the time that plasma cells were collected from the patients. The results for the 16 patients tested can be summarized as follows:
- 'A list of recommended drugs was provided to the patients’ oncologists and treatment choice was left to their discretion. FDA approval status, insurance coverage, prior treatment history, known side effect profiles, and patient preference were all factors considered in decision making. Combination therapies with drugs not included in the screening panel were allowed, and FDA approved drug doses were used regardless of HTS outcomes.’
- '13 of the 16 HTS patients received treatments that were recommended by HTS.’
- '92% of those patients achieved at least stable disease, with 31% partial responses and 15% very good partial responses. No complete responses were observed in this heavily pretreated group of patients.’
- ‘ … this work uncovered novel associations between genomic profiling data and drug sensitivity.’
- ‘The expression of 105 genes and mutations in 12 genes correlated with in vitro cytotoxicity.’
The researchers have also outlined plans for future development. They are expected to include a smaller number of drugs in their testing library so that fewer malignant cells need to be harvested which will increase the number of patients that may/will benefit from this technology. In addition, the larger patient population will allow the validation of the assay’s ability to predict clinical response. ‘Ongoing studies will also test therapeutic combinations, to reduce the opportunity for acquired drug resistance.’
Further fine-tuning of this technology may/will be of significant importance to us in the future, especially at time of relapse, when a drug treatment plan can be defined that is very specific to our specific individual clinical need. Something else to give us hope for the future.

about the author
Paul Kleutghen
I am a patient diagnosed in 2014 with primary plasma cell leukemia (pPCL), a rare and aggressive variant of multiple myeloma and have been very fortunate to find successful treatment at the division of Cellular Therapy at the Duke University Cancer Institute. My wife, Vicki, and I have two adult children and two grandsons who are the ‘lights of our lives’. Successful treatment has allowed Vicki and I to do what we love best : traveling the world, albeit it with some extra precautions to keep infections away. My career in the pharmaceutical industry has given me insights that I am currently putting to use as an advocate to lower drug pricing, especially prices for anti-cancer drugs. I am a firm believer that staying mentally active, physically fit, compliant to our treatment regimen and taking an active interest in our disease are keys to successful treatment outcomes.
More on Navigating Your Health





Trending Articles







Get the Latest Multiple Myeloma Updates, Delivered to You.
By subscribing to the HealthTree newsletter, you'll receive the latest research, treatment updates, and expert insights to help you navigate your health.
Together we care.
Together we cure.