Can Myelofibrosis Progress to Leukemia?

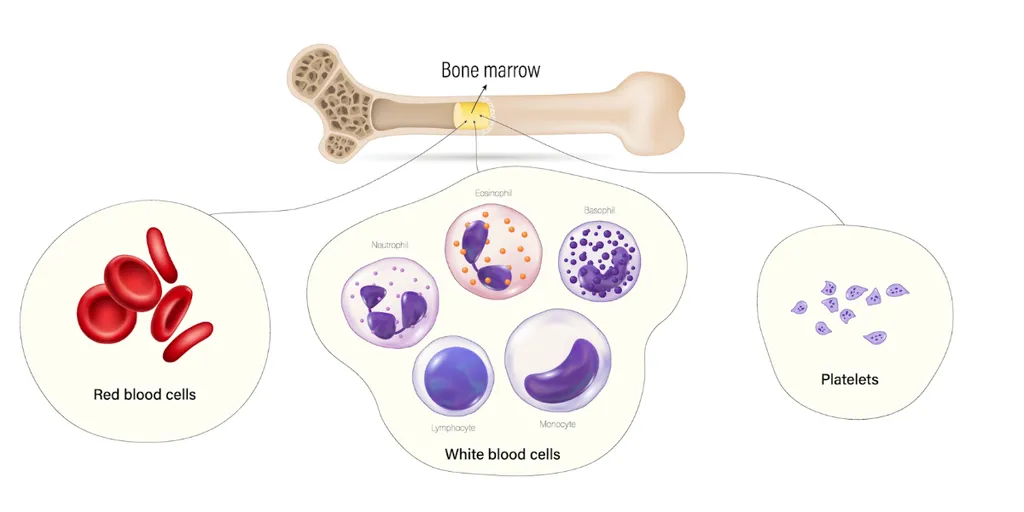
Myeloproliferative neoplasms (MPNs) are a group of blood disorders in which mature or immature bone marrow cells are overpopulated due to excessive blood cell production. Common symptoms of these disorders include fever, enlarged spleen, and a higher risk of blood clotting or bleeding issues.
The name of the myeloproliferative disorder is based on the type of cell involved. According to the NCI, myeloproliferative neoplasms include six subtypes:
- Myelofibrosis: The bone marrow forms abnormal blood cells and fibrous tissues.
- Chronic myeloid leukemia: overproduction of white blood cells in the bone marrow
- Polycythemia vera: overproduction of red blood cells in the bone marrow
- Essential thrombocythemia: overproduction of platelets in the bone marrow
- Chronic neutrophilic leukemia: The bone marrow overproduces neutrophils, a type of white blood cell.
- Chronic eosinophilic leukemia: The bone marrow overproduces eosinophils, another type of white blood cell.
When Leukemia Arises from Myeloproliferative Neoplasms, It’s Called Post-MPN or Secondary Acute Leukemia
Myeloproliferative neoplasms can progress to AML, which is called bast-phase myeloproliferative neoplasm. This is when excess blasts or immature blood cells are produced. It turns into AML when there are over 20% blasts in the bone marrow biopsy.
Approximately 5-10% of patients with myeloproliferative neoplasms will progress to AML. The most common type of MPN to progress is myelofibrosis. Approximately 20% of myelofibrosis patients will transform to AML in a 10-year period.
Some alterations in the bone marrow can be related to the appearance of leukemia. The risk of progressing varies by clinical, molecular, genetic, and laboratory values that are individual to every patient.
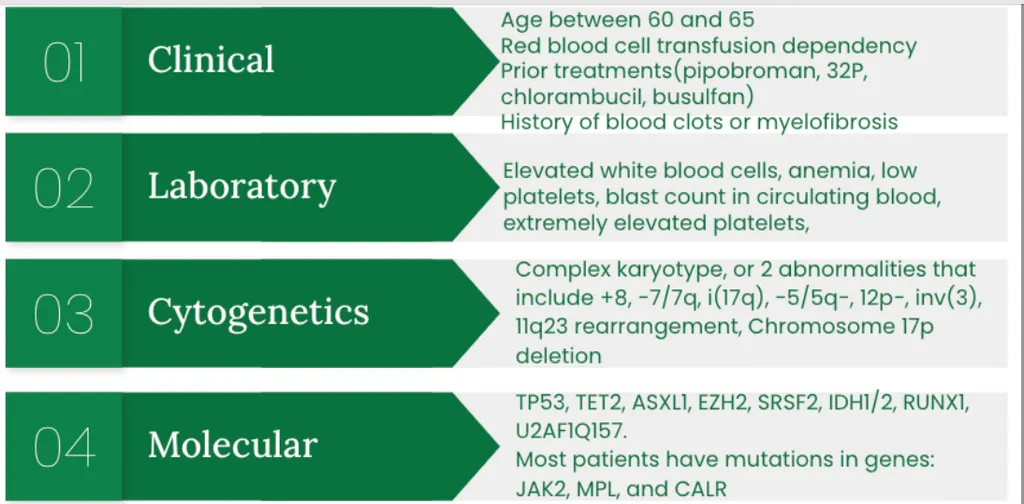
Compared to someone whose leukemia wasn’t due to a different disease, the genetics and appearance of leukemia cells under the microscope are different from someone who has myelofibrosis that transforms into leukemia.
Researchers must understand how a disease is formed to develop ways to stop it from forming in different pathways. A clear example is using JAK inhibitors, which stop the activity of enzymes in lymphocytes, the cells affected in leukemias.
Are Secondary Leukemias Treated Differently?
Despite a better understanding of molecular events in leukemias secondary to myelofibrosis or other bone marrow cancers, treatment outcomes for secondary AML have not improved significantly.
Standardizing treatments for secondary AML is still a challenge due to the multiple factors that can contribute to its formation.
The treatment options are tailored based on the patient's age and health status:
- Low-intensity therapies
- Standard AML regimens
- Allogeneic stem cell transplant: to date, is the only treatment option shown to have an impact on survival
- Vyxeos (Danorubicin and cytarabine) is an intravenous treatment for some types of secondary AML that can also be used in pediatric patients
Research is imperative to expand the treatment options for secondary AML since there are limited studies for this group of patients who progressed from myelofibrosis to leukemia.
You can contribute to life-saving research through HealthTree Cure Hub by creating an account!
Awareness of your health status, biweekly newsletter for your disease, access to clinical trial finder, and more leads to improved self-advocacy and disease outcomes!
Sources:
Myeloproliferative neoplasms (MPNs) are a group of blood disorders in which mature or immature bone marrow cells are overpopulated due to excessive blood cell production. Common symptoms of these disorders include fever, enlarged spleen, and a higher risk of blood clotting or bleeding issues.
The name of the myeloproliferative disorder is based on the type of cell involved. According to the NCI, myeloproliferative neoplasms include six subtypes:
- Myelofibrosis: The bone marrow forms abnormal blood cells and fibrous tissues.
- Chronic myeloid leukemia: overproduction of white blood cells in the bone marrow
- Polycythemia vera: overproduction of red blood cells in the bone marrow
- Essential thrombocythemia: overproduction of platelets in the bone marrow
- Chronic neutrophilic leukemia: The bone marrow overproduces neutrophils, a type of white blood cell.
- Chronic eosinophilic leukemia: The bone marrow overproduces eosinophils, another type of white blood cell.
When Leukemia Arises from Myeloproliferative Neoplasms, It’s Called Post-MPN or Secondary Acute Leukemia
Myeloproliferative neoplasms can progress to AML, which is called bast-phase myeloproliferative neoplasm. This is when excess blasts or immature blood cells are produced. It turns into AML when there are over 20% blasts in the bone marrow biopsy.
Approximately 5-10% of patients with myeloproliferative neoplasms will progress to AML. The most common type of MPN to progress is myelofibrosis. Approximately 20% of myelofibrosis patients will transform to AML in a 10-year period.
Some alterations in the bone marrow can be related to the appearance of leukemia. The risk of progressing varies by clinical, molecular, genetic, and laboratory values that are individual to every patient.
Compared to someone whose leukemia wasn’t due to a different disease, the genetics and appearance of leukemia cells under the microscope are different from someone who has myelofibrosis that transforms into leukemia.
Researchers must understand how a disease is formed to develop ways to stop it from forming in different pathways. A clear example is using JAK inhibitors, which stop the activity of enzymes in lymphocytes, the cells affected in leukemias.
Are Secondary Leukemias Treated Differently?
Despite a better understanding of molecular events in leukemias secondary to myelofibrosis or other bone marrow cancers, treatment outcomes for secondary AML have not improved significantly.
Standardizing treatments for secondary AML is still a challenge due to the multiple factors that can contribute to its formation.
The treatment options are tailored based on the patient's age and health status:
- Low-intensity therapies
- Standard AML regimens
- Allogeneic stem cell transplant: to date, is the only treatment option shown to have an impact on survival
- Vyxeos (Danorubicin and cytarabine) is an intravenous treatment for some types of secondary AML that can also be used in pediatric patients
Research is imperative to expand the treatment options for secondary AML since there are limited studies for this group of patients who progressed from myelofibrosis to leukemia.
You can contribute to life-saving research through HealthTree Cure Hub by creating an account!
Awareness of your health status, biweekly newsletter for your disease, access to clinical trial finder, and more leads to improved self-advocacy and disease outcomes!
Sources:

about the author
Jimena Vicencio
Jimena is an International Medical Graduate and a member of the HealthTree Writing team. She has a passion for languages and is currently learning Japanese. In her free time, she loves playing with her cats. Jimena is also pursuing a bachelor's degree in journalism.
More on Core Education








Get the Latest Essential Thrombocythemia Updates, Delivered to You.
By subscribing to the HealthTree newsletter, you'll receive the latest research, treatment updates, and expert insights to help you navigate your health.
Together we care.
Together we cure.