Understanding Your MDS Genetics

Understanding Your MDS Genetics
The genetic patterns found in MDS help us understand the impacts they have on the evolution and presentation of MDS. Genetics can help us to predict prognosis and focus on therapies for each mutation identified.
Myelodysplastic syndromes (MDS) are comprised of a diverse group of bone marrow disorders characterized by bone marrow failure resulting in abnormal cell creation and a high likelihood to progress to acute myeloid leukemia (AML).
Your bone marrow environment can be influenced by autoimmunity, chemotherapy, or radiation; all of these are known as extrinsic factors, and all of them can alter the way your DNA expresses. This damage to our DNA, or mutations, can lead to a defect in the production of normal bone marrow cells, instead creating cancer cells that multiply and grow faster than healthy normal cells, resulting in MDS.
Common Alterations: these are also targets for some MDS treatments
- DNA methylation (addition of a methyl group to the DNA, therefore modifying its structure)
- Chromatin modification (chromatin is the structure holding DNA in chromosomes, a modification can alter DNA)
- RNA splicing (Divisions in RNA that can lead to alterations in the protein production or cell functions)
- Transcription (the process that makes DNA give orders to RNA to produce something, it could be a protein or a cell signal)
- Signal transduction (the process that happens when cells react to substances outside the cell)
- Cohesin regulation (Cohesines make sure that the chromosomes stay ordered and put together, a mutation can be the product of troubled cohesin regulation)
- DNA repair (removal of damaged regions in the DNA).
How to read a genetics report
It is common to take a peek at a genetics lab report and see things like: del(18q), +21q gains. At first glance it may look like a typo or a jumbled up mess of letters, but it is just a a code of sorts that doctors use to simplify the reading of genetic findings. Let us unscramble it for you.
Del means deletion, + means addition, the number indicates which chromosome was affected, q means the long arm of the chromosome and p the petite or short arm of a chromosome.
So, back to our examples. Now we can understand that del(18q) is a deletion of the long arm of chromosome 18 and that +21q gains mean that the long arm of chromosome 21 had something added to it, meaning that maybe the arm got a little longer than it should be.
Chromosomes normally come in pairs of two. Sometimes however, a chromosome pair gains extra chromosomes, and they are no longer a pair anymore.
When the chromosome pair gains 1 new chromosome, totaling 3 chromosomes, it is called a trisomy. When the chromosome pair gains 2 new chromosomes, totaling 4 chromosomes, it is called a tetrasomy.
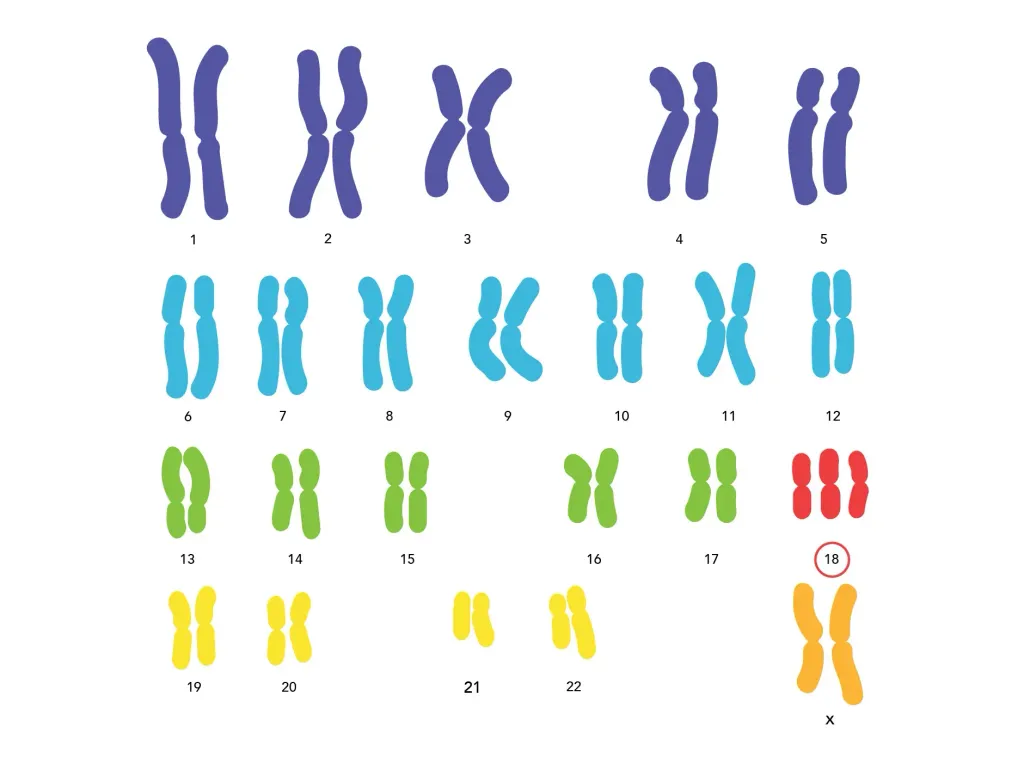
In the image, for example, there are 3 chromosomes in the 18th place, indicating that there is a trisomy in chromosome 18.
Another alteration that one may come across is a chromosome deletion like del(12p), that means that chromosome 12 lost its short arm or its whole pair, and there is only one chromosome 12 instead of a pair.
Driver Alteration In MDS
DRIVER is a term used to describe changes in the DNA that cause cells to become cancer cells and grow and spread throughout the body.
- Chromosomal and copy-number abnormalities; gains or losses of chromosomal materials.
- The most frequent are del(7q) and del(5q), followed by +8, dup(1q), del(20q), del(11q), del(12p)/t(12p), del(17p)/iso(17q), del(18q), +21q gains, del(13q), and +der(1;7)(q10;p10).
- Many of the lesions to the cell’s DNA happen at the same time as other complex abnormalities, designated as complex karyotypes. Involving multiple (≥3) chromosomes or chromosomal arms/segments, they are frequently accompanied by TP53 mutation (∼40% to 50%), generally predicting poor clinical outcomes, particularly when −5/del(5q) and del(17p) are involved.
- Rare cases (less than ∼2% to 3%) show recurrent reciprocal translocations, including t(3;21)(q26;q22), inv(3)(q21q26), t(3;3)(q21;q26), t(1;3)(q36;q21), and t(6;9)(q22;q34), which are associated with unique clinicopathological features and have high diagnostic values for MDS, even without clear evidence of myelodysplasia. Relevant driver genes include MPL and NRAS (1pUPD), TET2 (4qLOH), CUX1 and EZH2 (7qLOH), CBL (11qLOH), ETV6 (del(12p)), FLT3 (13qUPD), TP53 (17pLOH), and RUNX1 (21qLOH).
Genetic mutations are frequently associated with specific disease presentation, drug response, and clinical outcomes. That’s why it's essential to be familiar with your MDS genetics and for physicians to run tests so they can better identify the most effective treatment.
What are the tests for genetic mutations?
- NGS or next-generation sequencing specifically reviews our DNA sequence and can identify genetic mutations.
- Karyotype: ordering the chromosomes and identifying chromosomal abnormalities (morphological or numerical alteration in single or multiple chromosomes)
- FISH fluorescent in situ hybridization a test made to find specific mutations in the damaged cells, the test is positive if the mutation glows fluorescent. (In the image we can see how the chromosomes glow fluorescent and the color red, is not showing up its pair in del5q) because the long arm of chromosome 5 got a deletion.
- SNP single nucleotide polymorphism; it’s a change of order in a sequence of nucleotides (chains that make up our DNA), this test can detect chromosomal copy-number abnormalities and also copy-neutral loss of heterozygocity meaning that 2 copies from a chromosome come from the same parent cell, and the DNA material is not mixing up being this way more prone to alterations.
What do I do with this information?
Ask questions, work with your attending physician, and participate in trials.
The human genome is larger than any library, and has more information than any database. MDS patients alone carry a median of 1500 mutations across the entire genome (Yasuhito Nannya and the MDS Whole Genome Project, unpublished observation).
It is challenging to understand even for the most skilled physician. It’s important for you as a patient or as a caregiver to understand that your MDS diagnosis has to be tested for a more accurate, tailor-made treatment. The genetics underlying MDS are key to finding an effective cure. Even though many of these genetic abnormalities have been identified, researchers keep looking in that direction to hopefully one day figure out a way to avoid them.
Understanding Your MDS Genetics
The genetic patterns found in MDS help us understand the impacts they have on the evolution and presentation of MDS. Genetics can help us to predict prognosis and focus on therapies for each mutation identified.
Myelodysplastic syndromes (MDS) are comprised of a diverse group of bone marrow disorders characterized by bone marrow failure resulting in abnormal cell creation and a high likelihood to progress to acute myeloid leukemia (AML).
Your bone marrow environment can be influenced by autoimmunity, chemotherapy, or radiation; all of these are known as extrinsic factors, and all of them can alter the way your DNA expresses. This damage to our DNA, or mutations, can lead to a defect in the production of normal bone marrow cells, instead creating cancer cells that multiply and grow faster than healthy normal cells, resulting in MDS.
Common Alterations: these are also targets for some MDS treatments
- DNA methylation (addition of a methyl group to the DNA, therefore modifying its structure)
- Chromatin modification (chromatin is the structure holding DNA in chromosomes, a modification can alter DNA)
- RNA splicing (Divisions in RNA that can lead to alterations in the protein production or cell functions)
- Transcription (the process that makes DNA give orders to RNA to produce something, it could be a protein or a cell signal)
- Signal transduction (the process that happens when cells react to substances outside the cell)
- Cohesin regulation (Cohesines make sure that the chromosomes stay ordered and put together, a mutation can be the product of troubled cohesin regulation)
- DNA repair (removal of damaged regions in the DNA).
How to read a genetics report
It is common to take a peek at a genetics lab report and see things like: del(18q), +21q gains. At first glance it may look like a typo or a jumbled up mess of letters, but it is just a a code of sorts that doctors use to simplify the reading of genetic findings. Let us unscramble it for you.
Del means deletion, + means addition, the number indicates which chromosome was affected, q means the long arm of the chromosome and p the petite or short arm of a chromosome.
So, back to our examples. Now we can understand that del(18q) is a deletion of the long arm of chromosome 18 and that +21q gains mean that the long arm of chromosome 21 had something added to it, meaning that maybe the arm got a little longer than it should be.
Chromosomes normally come in pairs of two. Sometimes however, a chromosome pair gains extra chromosomes, and they are no longer a pair anymore.
When the chromosome pair gains 1 new chromosome, totaling 3 chromosomes, it is called a trisomy. When the chromosome pair gains 2 new chromosomes, totaling 4 chromosomes, it is called a tetrasomy.
In the image, for example, there are 3 chromosomes in the 18th place, indicating that there is a trisomy in chromosome 18.
Another alteration that one may come across is a chromosome deletion like del(12p), that means that chromosome 12 lost its short arm or its whole pair, and there is only one chromosome 12 instead of a pair.
Driver Alteration In MDS
DRIVER is a term used to describe changes in the DNA that cause cells to become cancer cells and grow and spread throughout the body.
- Chromosomal and copy-number abnormalities; gains or losses of chromosomal materials.
- The most frequent are del(7q) and del(5q), followed by +8, dup(1q), del(20q), del(11q), del(12p)/t(12p), del(17p)/iso(17q), del(18q), +21q gains, del(13q), and +der(1;7)(q10;p10).
- Many of the lesions to the cell’s DNA happen at the same time as other complex abnormalities, designated as complex karyotypes. Involving multiple (≥3) chromosomes or chromosomal arms/segments, they are frequently accompanied by TP53 mutation (∼40% to 50%), generally predicting poor clinical outcomes, particularly when −5/del(5q) and del(17p) are involved.
- Rare cases (less than ∼2% to 3%) show recurrent reciprocal translocations, including t(3;21)(q26;q22), inv(3)(q21q26), t(3;3)(q21;q26), t(1;3)(q36;q21), and t(6;9)(q22;q34), which are associated with unique clinicopathological features and have high diagnostic values for MDS, even without clear evidence of myelodysplasia. Relevant driver genes include MPL and NRAS (1pUPD), TET2 (4qLOH), CUX1 and EZH2 (7qLOH), CBL (11qLOH), ETV6 (del(12p)), FLT3 (13qUPD), TP53 (17pLOH), and RUNX1 (21qLOH).
Genetic mutations are frequently associated with specific disease presentation, drug response, and clinical outcomes. That’s why it's essential to be familiar with your MDS genetics and for physicians to run tests so they can better identify the most effective treatment.
What are the tests for genetic mutations?
- NGS or next-generation sequencing specifically reviews our DNA sequence and can identify genetic mutations.
- Karyotype: ordering the chromosomes and identifying chromosomal abnormalities (morphological or numerical alteration in single or multiple chromosomes)
- FISH fluorescent in situ hybridization a test made to find specific mutations in the damaged cells, the test is positive if the mutation glows fluorescent. (In the image we can see how the chromosomes glow fluorescent and the color red, is not showing up its pair in del5q) because the long arm of chromosome 5 got a deletion.
- SNP single nucleotide polymorphism; it’s a change of order in a sequence of nucleotides (chains that make up our DNA), this test can detect chromosomal copy-number abnormalities and also copy-neutral loss of heterozygocity meaning that 2 copies from a chromosome come from the same parent cell, and the DNA material is not mixing up being this way more prone to alterations.
What do I do with this information?
Ask questions, work with your attending physician, and participate in trials.
The human genome is larger than any library, and has more information than any database. MDS patients alone carry a median of 1500 mutations across the entire genome (Yasuhito Nannya and the MDS Whole Genome Project, unpublished observation).
It is challenging to understand even for the most skilled physician. It’s important for you as a patient or as a caregiver to understand that your MDS diagnosis has to be tested for a more accurate, tailor-made treatment. The genetics underlying MDS are key to finding an effective cure. Even though many of these genetic abnormalities have been identified, researchers keep looking in that direction to hopefully one day figure out a way to avoid them.

about the author
Jimena Vicencio
Jimena is an International Medical Graduate and a member of the HealthTree Writing team. She has a passion for languages and is currently learning Japanese. In her free time, she loves playing with her cats. Jimena is also pursuing a bachelor's degree in journalism.
More on Navigating Your Health






Trending Articles




Get the Latest Myelodysplastic Syndromes Updates, Delivered to You.
By subscribing to the HealthTree newsletter, you'll receive the latest research, treatment updates, and expert insights to help you navigate your health.
Together we care.
Together we cure.