With Coach, we are in this together
HealthTree Coaches are experienced patients and caregivers who understand the importance of support from someone who knows first-hand what you’re going through.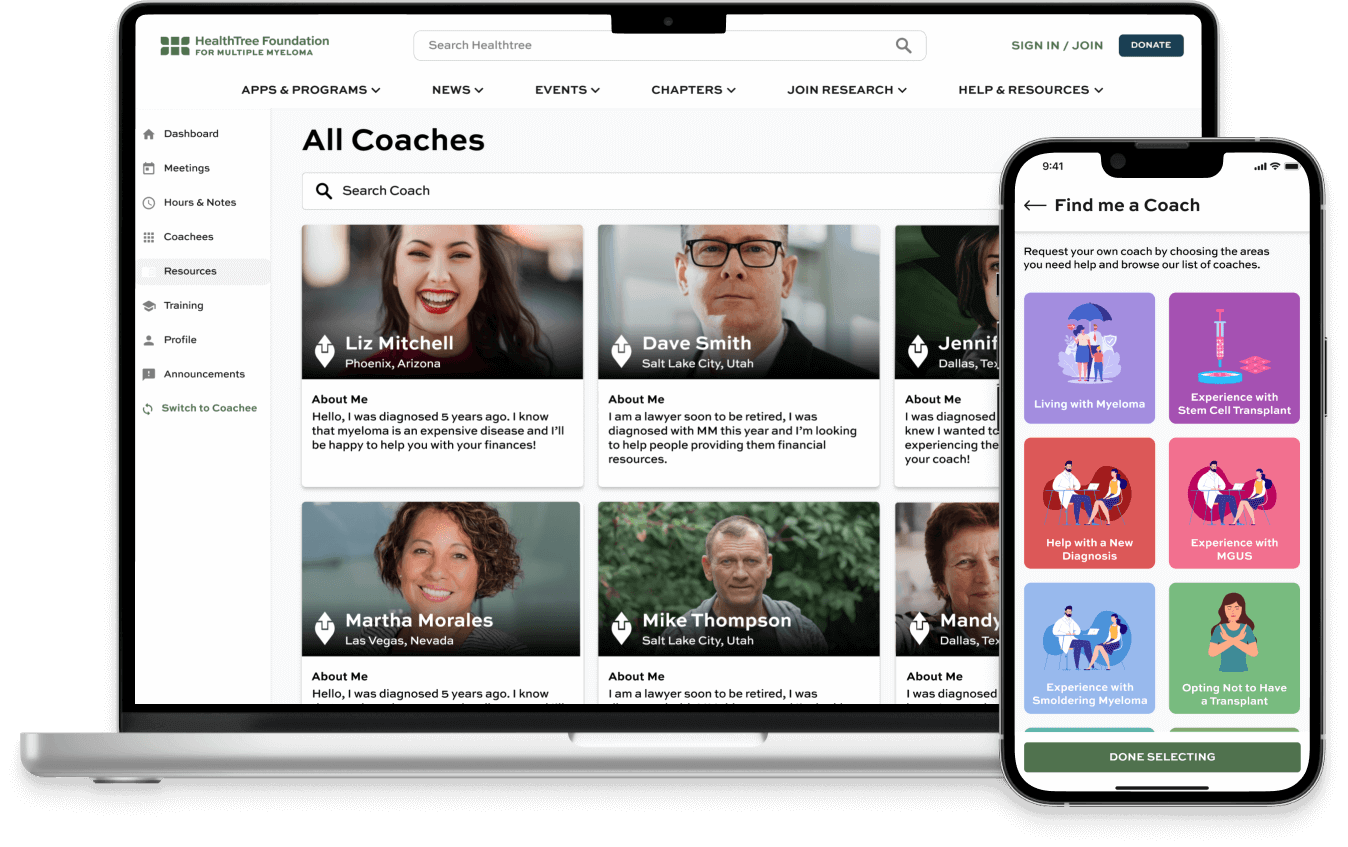
Personalized Coaching
All Coaches are volunteer survivors or caregivers who want to share their experiences and help guide you through your diagnosis and treatment.You can find a coach who:
- Has your type of disease
- Had a similar treatment
- Has personal areas of experience to match your needs
- Lives in your geographic area
You are able to work with more than one Coach at a time and can connect by phone, computer
or in person.
Become a Coach
- Make a meaningful difference in patients' lives.
- No experience needed – we provide comprehensive training on skills and knowledge to help you succeed.
- Commitment - Dedicate at least 8 hours per month for one year.
- Access to easy-to-use resources, including online videos, webinars, and helpful tools to help you find the right answers quickly.
Find Meaningful Connections


Thanks to our sponsors:




